

 PDF
PDF ePub
ePub Citation
Citation Print
Print


Abstract
It is extremely rare to observe ossifying lipoma that developes separately from bone tissues in the groin. A patient with an adult fist-sized, firm, non-movable and painless mass in the left groin area, had been treated with marginal excision, which turned out to be ossifying lipoma. Although many different variants of lipoma with bone tissue have been reported, a case like this has never previously been reported. It is important to distinguish ossifying lipoma, from tumors with calcific lesions. We report its uniqueness in radiologic and pathologic ways, with specific findings of ossifying lipoma.
Figures and Tables
Figure 1
The simple radiography images show a man's fist sized mass with shell like calcification in the left groin area without connected to the bone.

Figure 2
The bone scan image of round and well-demarcated hot uptake lesion on trochanteric area of left femur.

Figure 3
The axial computed tomography (CT) image shows a well defined peripheral rim of calcification surrounding the ossified mass.
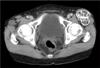
Figure 4
(A) The axial T1-weighted magnetic resonance (MR) shows a lobulated mass anterolaterally to the femoral head with high signal intensity similar to that of subcutaneous. (B) The axial T2-weighted MR image shows a lobulated mass with heterogenous signal intensity. (C) The axial T1-weighted enhanced MR image shows a moderately increased signal intensity of a mass.

Figure 5
The pathologic specimen of the excised ossifying lipoma. (A) Well-circumscribed two-lobed hard mass (6.5×5.5×3.5 cm) shows a smooth ivory-colored surface. (B) Greasy and gritty bone marrow-like cut surface.

Figure 6
Histologic examinations of the tumor. (A) Thin layer of the lamellar bone constitutes the peripheral portion of the tumor (H&E, ×40). (B) The inner portion of the tumor is composed of fat tissue and interspersed trabeculae of lamellar bone (H&E, ×100). (C) There was no evidence of nuclear atypia, hypercellularity, mitosis and necrosis (H&E, ×250).

References
1. Mentzel T. Lipomatous tumors of the skin and soft tissue. New entities and concepts. Pathologe. 2000. 21:441–448.
2. Heffernan EJ, Lefaivre K, Munk PL, Nielsen TO, Masri BA. Ossifying lipoma of the thigh. Br J Radiol. 2008. 81:e207–e210.
3. Plaut GS, Salm R, Truscott DE. Three cases of ossifying lipoma. J Pathol Bacteriol. 1959. 78:292–295.

4. Demiralp B, Alderete JF, Kose O, Ozcan A, Cicek I, Basbozkurt M. Osteolipoma independent of bone tissue: a case report. Cases J. 2009. 2:8711.
5. Fritchie KJ, Renner JB, Rao KW, Esther RJ. Osteolipoma: radiological, pathological, and cytogenetic analysis of three cases. Skeletal Radiol. 2012. 41:237–244.
6. Gaskin CM, Helms CA. Lipomas, lipoma variants, and well-differentiated liposarcomas (atypical lipomas): results of MRI evaluations of 126 consecutive fatty masses. AJR Am J Roentgenol. 2004. 182:733–739.
7. Obermann EC, Bele S, Brawanski A, Knuechel R, Hofstaedter F. Ossifying lipoma. Virchows Arch. 1999. 434:181–183.
8. Bispo RZ Junior, Guedes AV. Parosteal lipoma of the femur with hyperostosis: case report and literature review. Clinics (Sao Paulo). 2007. 62:647–652.
9. Rodriguez-Peralto JL, Lopez-Barea F, Gonzalez-Lopez J, Lamas-Lorenzo M. Case report 821: Parosteal ossifying lipoma of femur. Skeletal Radiol. 1994. 23:67–69.
10. Val-Bernal JF, Val D, Garijo MF, Vega A, González-Vela MC. Subcutaneous ossifying lipoma: case report and review of the literature. J Cutan Pathol. 2007. 34:788–792.
 XML Download
XML Download