

 PDF
PDF ePub
ePub Citation
Citation Print
Print


Abstract
Purpose
Most humeral fractures of children are treated satisfactorily with conservative method, thus surgical treatment is often reserved for limited conditions. In cases of an open fracture, inadequate reduction or multiple traumas, children with humeral shaft fractures require operative treatment. The aim of our study was to evaluate results and complications of pediatric humeral shaft fractures that were treated with flexible intramedullary nails.
Materials and Methods
A retrospective study was performed for 12 patients who were treated operatively by flexible intramedullary nails between March 2009 and September 2011. Surgical indications were an open fracture, an inability to maintain an adequate reduction, concomitant fractures, refractures and combined radial nerve injury. All patients were treated with 2 titanium flexible intramedullary nails by antegrade or retrograde techniques, according to the site of the fractures.
Results
The mean follow-up period was 15 months, and all patients achieved union status without major complications. There were no neurovascular injuries or infection during surgical procedures. However, 4 patients showed irritation at the insertion site of the nail, and 2 of them underwent early removal of nails at about 6 weeks due to skin lesions as well as pain and discomfort. One boy showed a fracture next to the proximal insertion site of the antegrade nail. All patients showed a full range of motion, and went back to daily life by the final follow-up.
Figures and Tables
 | Figure 1 Patient 12. (A) Anteroposterior radiograph of the humerus with proximal 1/3 shaft fracture. (B) Fracture was stabilized with 2 titanium elastic nails by 2 lateral retrograde insertions.
|
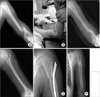 | Figure 2Patient 1. (A-C) A 12-year-old boy with distal 1/3 shaft fracture of the humerus. It was an open fracture and reduction was not maintained by closed method. (D) Fracture was stabilized with 2 nails by antegrade insertion. (E) After 6 months, there was fracture next to insertion site by minor injury. (F) Anteroposterior radiograph showed fracture union with conservative treatment.
|
 | Figure 3Patient 9. (A) Reduction was maintained by closed method and U plaster. (B) After 6 weeks, this 10-year-old boy was hit by his friend and refracture happened. (C) Fracture was fixed with 2 titanium elastic nails. (D) After 13 months, anteroposterior radiograph showed well union status without complications.
|

References
1. Cheng JC, Shen WY. Limb fracture pattern in different pediatric age groups: a study of 3,350 children. J Orthop Trauma. 1993. 7:15–22.
2. Beaty JH, Kasser JR. Rockwood and Wilkins' Fractures in Children. 2010. 7th ed. Philadelphia: Lippincott;656–667.
3. Brumback RJ, Bosse MJ, Poka A, Burgess AR. Intramedullary stabilization of humeral shaft fractures in patients with multiple trauma. J Bone Joint Surg Am. 1986. 68:960–970.

4. Hennigan SP, Bush-Joseph CA, Kuo KN, Bach BR Jr. Throw-ing-induced humeral shaft fracture in skeletally immature adolescents. Orthopedics. 1999. 22:621–622.
5. Beringer DC, Weiner DS, Noble JS, Bell RH. Severely dis-placed proximal humeral epiphyseal fractures: a follow-up study. J Pediatr Orthop. 1998. 18:31–37.
6. Hohl JC. Fractures of the humerus in children. Orthop Clin North Am. 1976. 7:557–571.
7. Chapman JR, Henley MB, Agel J, Benca PJ. Randomized prospective study of humeral shaft fracture fixation: intramedullary nails versus plates. J Orthop Trauma. 2000. 14:162–166.
8. Shazar N, Brumback RJ, Vanco B. Treatment of humeral fractures by closed reduction and retrograde intramedullary Ender nails. Orthopedics. 1998. 21:641–646.
9. Williams PR, Shewring D. Use of an elastic intramedullary nail in difficult humeral fractures. Injury. 1998. 29:661–670.
10. Dietz HG, Schmittenbecher PP, Slongo T, Wilkins KE. Elastic stable intramedullary nailing (ESIN) in children (AO manual of fracture management series). 2006. Switzerland: Thieme;20–43.
11. Zehms CT, Balsamo L, Dunbar R. Coaptation splinting for humeral shaft fractures in adults and children: a modified method. Am J Orthop (Belle Mead NJ). 2006. 35:452–454.
12. Hutchinson PH, Bae DS, Waters PM. Intramedullary nailing versus percutaneous pin fixation of pediatric proximal humerus fractures: a comparison of complications and early radiographic results. J Pediatr Orthop. 2011. 31:617–622.
13. Mackay I. Closed Rush pinning of fractures of the humeral shaft. Injury. 1984. 16:178–181.
14. Stern PJ, Mattingly DA, Pomeroy DL, Zenni EJ Jr, Kreig JK. Intramedullary fixation of humeral shaft fractures. J Bone Joint Surg Am. 1984. 66:639–646.
15. Machan FG, Vinz H. Humeral shaft fracture in childhood. Unfallchirurgie. 1993. 19:166–174.
16. Packer JW, Foster RR, Garcia A, Grantham SA. The humeral fracture with radial nerve palsy: is exploration warranted? Clin Orthop Relat Res. 1972. 88:34–38.
17. Shah JJ, Bhatti NA. Radial nerve paralysis associated with fractures of the humerus A review of 62 cases. Clin Orthop Relat Res. 1983. 172:171–176.
18. Vukadinović S, Mikić Z, Lartey J. Humeral fractures complicated by radial nerve lesions. Acta Chir Iugosl. 1981. 28:211–217.
19. Garg S, Dobbs MB, Schoenecker PL, Luhmann SJ, Gordon JE. Surgical treatment of traumatic pediatric humeral di-aphyseal fractures with titanium elastic nails. J Child Orthop. 2009. 3:121–127.
 XML Download
XML Download