

 PDF
PDF ePub
ePub Citation
Citation Print
Print


Abstract
Purpose
To evaluate clinical outcomes of triscaphe (STT), scapho-capitate (SC) and scapho-capito-hamato-triquetral (SCHT) fusion in advanced Kienböck's disease.
Materials and Methods
Forty patients with Lichtman stage III and IV disease were treated with limited wrist fusion. STT & SC fusion for stage IIIa and IIIb, and SCHT fusion for IIIb and IV were done according to preoperative radiologic and intraoperative articular surface findings. The mean follow-up period was 31.6 months (range 13-108) and the mean age at the time of their surgery was 44.7 years (range 22-71). There were 13 cases of STT fusion, 19 cases of SC fusion and 8 cases of SCHT fusion. For assessment of treatment results, wrist range of motion, grip strength, VAS (visual analog pain score) and any radiologic changes of the wrist were checked at last follow-up.
Results
VAS score was 4.7 for STT, 3.0 for SC, 4.5 for SCHT. Grip strength, compared with the contralateral side, was 72% for STT, 78% for SC, and 54% for SCHT. Pain was more improved for the SC fusion group than for the other two groups (p=0.007). Grip strength was decreased more in the SCHT fusion group than in the other two groups (p=0.009). There were no statistically significant differences in range of motion between any of the three groups. The bone achieved union in all cases except one SC fusion.
Conclusion
Limited wrist fusion in advanced Kienböck's disease has been regarded as a valuable method. However, SC fusion has been thought of as a more favorable technique than STT fusion with respect to pain relief. SCHT fusion is thought to be a possible salvage procedure with a limited indication for Stage IV Kienböck's disease.
Figures and Tables
Figure 1
(A) Schematic image of the scapho-capito-hamato-triquetral fusion. (B) Scapholunate angle is about 45 degrees.

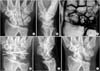
Figure 2
A 36-year-old woman with Kienböck's disease. (A, B) Preoperative plain radiographs show collapsed lunate, but scapholunate angle is within normal range (Lichtman IIIa). (C) Magnetic resonance image shows avascular necrosis of the lunate. (D, E) Postoperative plain radiographs. (F) Twenty five months after scapho-capitate fusion, patient was relieved from the wrist pain and preserved some wrist motions.
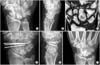
Figure 3
A 50-year-old man with Kienböck's disease. (A, B) Preoperative plain radiograph shows carpal collapse, lunate fragmentation and scaphoid rotational deformity. (C) Magnetic resonance image shows midcarpal joint arthritic change. (D, E) Postoperative plain radiographs. (F) Sixteen months after the scapho-capito-hamato-triquetral fusion, patient was improved from pain, and still preserved some radiocarpal joint motions.



References
1. Blanco RH. Excision of the lunate in Kienböck's disease: long-term results. J Hand Surg Am. 1985. 10:1008–1013.

2. Ishiguro T. Experimental and clinical studies of Kienböck's disease. Excision of the lunate followed by packing of the free tendon. Nippon Seikeigeka Gakkai Zasshi. 1984. 58:509–522.
3. Almquist EE. Kienböck's disease. Hand Clin. 1987. 3:141–148.
4. Horii E, Garcia-Elias M, Bishop AT, Cooney WP, Linscheid RL, Chao EY. Effect on force transmission across the carpus in procedures used to treat Kienböck's disease. J Hand Surg Am. 1990. 15:393–400.
5. Almquist EE, Burns JF Jr. Radial shortening for the treatment of Kienböck's disease--a 5- to 10-year follow-up. J Hand Surg Am. 1982. 7:348–352.
6. Quenzer DE, Dobyns JH, Linscheid RL, Trail IA, Vidal MA. Radial recession osteotomy for Kienböck's disease. J Hand Surg Am. 1997. 22:386–395.
7. Weiss AP, Weiland AJ, Moore JR, Wilgis EF. Radial shortening for Kienböck's disease. J Bone Joint Surg Am. 1991. 73:384–391.
8. Iwasaki N, Genda E, Barrance PJ, Minami A, Kaneda K, Chao EY. Biomechanical analysis of limited intercarpal fusion for the treatment of Kienböck's disease: a three-dimensional theoretical study. J Orthop Res. 1998. 16:256–263.
9. Sauerbier M, Kluge S, Bickert B, Germann G. Subjective and objective outcomes after total wrist arthrodesis in patients with radiocarpal arthrosis or Kienböck's disease. Chir Main. 2000. 19:223–231.
10. Jorgensen EC. Proximal-row carpectomy. An end-result study of twenty-two cases. J Bone Joint Surg Am. 1969. 51:1104–1111.
11. Watson HK, Ryu J. Evolution of arthritis of the wrist. Clin Orthop Relat Res. 1986. 202:57–67.
12. Watson HK, Weinzweig J, Guidera PM, Zeppieri J, Ashmead D. One thousand intercarpal arthrodeses. J Hand Surg Br. 1999. 24:307–315.
13. Watson HK, Ryu J, DiBella A. An approach to Kienböck's disease: triscaphe arthrodesis. J Hand Surg Am. 1985. 10:179–187.
14. Meier R, van Griensven M, Krimmer H. Scaphotrapeziotrapezoid (STT)-arthrodesis in Kienböck's disease. J Hand Surg Br. 2004. 29:580–584.
15. Yoon JH, Kim EG, Cha YC. Triscaphe fusion with radial styloidectomy in Kienböck's disease. J Korean Orthop Assoc. 1998. 33:1816–1821.
16. Sauerbier M, Tränkle M, Erdmann D, Menke H, Germann G. Functional outcome with scaphotrapeziotrapezoid arthrodesis in the treatment of Kienböck's disease stage III. Ann Plast Surg. 2000. 44:618–625.
17. Fortin PT, Louis DS. Long-term follow-up of scaphoid-trapezium-trapezoid arthrodesis. J Hand Surg Am. 1993. 18:675–681.
18. Kleinman WB, Carroll C 4th. Scapho-trapezio-trapezoid arthrodesis for treatment of chronic static and dynamic scapho-lunate instability: a 10-year perspective on pitfalls and complications. J Hand Surg Am. 1990. 15:408–414.
19. Watson HK, Monacelli DM, Milford RS, Ashmead D IV. Treatment of Kienböck's disease with scaphotrapeziotrapezoid arthrodesis. J Hand Surg Am. 1996. 21:9–15.
20. Frykman EB, Af Ekenstam F, Wadin K. Triscaphoid arthrodesis and its complications. J Hand Surg Am. 1988. 13:844–849.
21. Pisano SM, Peimer CA, Wheeler DR, Sherwin F. Scaphocapitate intercarpal arthrodesis. J Hand Surg Am. 1991. 16:328–333.
22. Sennwald GR, Ufenast H. Scaphocapitate arthrodesis for the treatment of Kienböck's disease. J Hand Surg Am. 1995. 20:506–510.
23. Short WH, Werner FW, Fortino MD, Palmer AK. Distribution of pressures and forces on the wrist after simulated intercarpal fusion and Kienböck's disease. J Hand Surg AM. 1992. 17:443–449.
24. Trumble T, Glisson RR, Seaber AV, Urbaniak JR. A biomechanical comparison of the methods for treating Kienböck's disease. J Hand Surg Am. 1986. 11:88–93.
25. Moy OJ, Peimer CA. Scaphocapitate fusion in the treatment of Kienböck's disease. Hand Clin. 1993. 9:501–504.
26. Takase K, Imakiire A. Lunate excision, capitate osteotomy, and intercarpal arthrodesis for advanced Kienböck disease. Long-term follow-up. J Bone Joint Surg Am. 2001. 83-A:177–183.
 XML Download
XML Download