

 PDF
PDF ePub
ePub Citation
Citation Print
Print


Abstract
Purpose
This study examined the obstacles preventing a decrease in a facet joint fracture-dislocation of the lower cervical spine after skeletal traction to determine suitable treatment guidelines.
Materials and Methods
This study examined 19 fracture-dislocation cases of the facet joint in the lower cervical spine who failed closed reduction through skeletal traction. The following parameters were analyzed: obstacles preventing reduction, neurological recovery, complications and body to canal ratio of the injured site.
Results
The obstacles found on MRI were herniated discs in 17 cases and joint capsule in 2 cases. The surgical decision was based on an analysis of the size and location of the disc, the degree of spinal canal stenosis and damage of the posterior structures. Anterior reduction/fusion and posterior fusion after anterior reduction/fusion, anterior fusion after posterior reduction/fusion and posterior reduction/fusion was performed in 9, 2, 6 and 2 cases, respectively. There was significant neurological recovery at the final follow-up (p=0.000). The body to canal ratio also increased significantly after surgery (p=0.000).
Conclusion
For the treatment of unreducible facet joint fracture-dislocation of the cervical spine, pre-reduction MRI is essential for a thorough evaluation of the various underlying pathologies. In addition the surgical methods should be determined according to not only the neurological status, obstacles and pathologic structures preventing reduction, but also the surgeon's experience.
Figures and Tables
Figure 1
(A) Preoperative cervical lateral plain radiogram shows bilateral locked facets on C6-7 and the fracture of the anterosuperior portion of the C7 vertebral body of a 60-year-old man who suffered from complete cord injury due to motorcycle accident. (B) Preoperative sagittal and axial MR images show ruptured disc fragment under the posterior of the vertebral body and posterior longitudinal ligament as a cause of reduction failure. (C) Intraoperative cervical lateral plain radiogram of the patient under a 50lb Gardner-Well skull traction shows the unreduced state of dislocated facets. (D) Postoperative cervical lateral radiogram shows the good reduction by the posterior reduction and fixation/fusion method, after anterior discectomy and fixation/fusion.

Figure 2
(A) Preoperative cervical lateral plain radiogram shows bilateral locked facets on C5-6 of a 57-year-old man who suffered from incomplete cord injury due to pedestrian traffic accident. (B) Preoperative sagittal and axial MR images show ruptured disc fragment under the uncovertebral joint and posterior longitudinal ligament as a cause of reduction failure. (C) Preoperative cervical lateral plain radiogram of the patient under a 50lb Gardner-Well skull traction shows the unreduced state of dislocated facets. (D) Intraoperative cervical lateral plain radiogram of the patient under a 50lb Gardner-Well skull traction shows the reduced state of dislocated facets. (E) Postoperative cervical lateral radiogram shows the good reduction by the anterior discectomy and fixation/fusion.

Figure 3
(A) Preoperative cervical lateral plain radiogram shows unilateral locked facets on C3-4 of a 34-year-old man who suffered from radiculopathy due to driver accident. (B) Preoperative sagittal and axial MR images show no prolapse of disc material on C3-4. (C) Intraoperative cervical lateral plain radiogram of the patient under a 50lb Gardner-Well skull traction shows the reduced state of dislocated facets. (D) Postoperative cervical lateral radiogram shows the good reduction by the posterior reduction and fixation/fusion method.
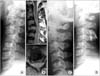
Table 1
Data of Patient's Profile

*Initial neurologic status; †Obstacles of reduction; ‡Preoperative Pavlov ratio; §Postoperative Pavlov ratio; ∥Preoperative motor ASIA score; ¶Postoperative motor ASIA score; **Last follow-up motor ASIA score; ††Preoperative sensory ASIA score; ‡‡Postoperative sensory ASIA score; §§Last follow-up sensory ASIA score.
R, Radiculopathy; ICI, Incomplete cord injury; CCI, Complete cord injury; AF, Anterior cervical discectomy and fusion; PS, Posterior stabilization; LF, Locked facet.
References
1. Vaccaro AR, Madigan L, Schweitzer ME, Flanders AE, Hilibrand AS, Albert TJ. Magnetic resonance imaging analysis of soft tissue disruption after flexion-distraction injuries of the subaxial cervical spine. Spine (Phila Pa 1976). 2001. 17:1866–1872.

2. Schaefer DM, Fladers A, Northrup BE, Doan HT, Osterholm JL. Magnetic resonance imaging of acute cervical spine trauma. Correlation with severity of neurologic injury. Spine (Phila Pa 1976). 1989. 14:1090–1095.
3. Robinson RA, Smith GW. Anterolateral cervical disk removal and interbody fusion for cervical disk syndrome. Bull Johns Hopkins Hosp. 1955. 96:223–224.
4. de Oliveira JC. Anterior reduction of interlocking facets in the lower cervical spine. Spine (Phila Pa 1976). 1979. 4:195–202.
5. Reindl R, Ouellet J, Harvey EJ, Berry G, Arlet V. Anterior reduction for cervical spine dislocation. Spine (Phila Pa 1976). 2006. 31:648–652.
6. Kleyn PJ. Dislocations of the cervical spine: closed reduction under anaesthesia. Paraplegia. 1984. 22:271–281.
7. Mirza SK, Krengel WF 3rd, Chapman JR, et al. Early versus delayed surgery for acute cervical spinal cord injury. Clin Orthop Relat Res. 1999. 359:104–114.
8. Rorabeck CH, Rock MG, Hawkins RJ, Bourne RB. Unilateral facet dislocation of the cervical spine. An analysis of the results of treatment in 26 patients. Spine (Phila Pa 1976). 1987. 12:23–27.
9. Grant GA, Mirza SK, Chapman JR, et al. Risk of early closed reduction in cervical spine subluxation injuries. J Neurosurg. 1999. 90:1 Suppl. 13–18.
10. Rizzolo SJ, Vaccaro AR, Cotler JM. Cervical spine trauma. Spine (Phila Pa 1976). 1994. 19:2288–2298.
11. Cotler JM, Herbison GJ, Nasuti JF, Ditunno JF Jr, An H, Wolff BE. Closed reduction of traumatic cervical spine dislocation using traction weights up to 140 pounds. Spine (Phila Pa 1976). 1993. 18:386–390.
12. Braakman R, Vinken PJ. Unilateral facet interlocking in the lower cervical spine. J Bone Joint Surg Br. 1967. 49:249–257.
13. Pratt ES, Green DA, Spengler DM. Herniated intervertebral discs associated with unstable spinal injuries. Spine (Phila Pa 1976). 1990. 15:662–666.
14. Payer M. Immediate open anterior reduction and antero-posterior fixation/fusion for bilateral cervical locked facets. Acta Neurochir (Wien). 2005. 147:509–514.
15. Bailey RW, Badgley CE. Stabilization of the cervical spine by anterior fusion. J Bone Joint Surg Am. 1960. 42:565–594.
16. Stauffer ES, Rhoades ME. Surgical stabilization of the cervical spine after trauma. Arch Surg. 1976. 111:652–657.
17. Capen DA, Garland DE, Waters RL. Surgical stabilization of the cervical spine. A comparative analysis of anterior and posterior spine fusions. Clin Orthop Relat Res. 1985. 196:229–237.
18. Song KJ, Ji JH, Hwang BY. Disc extrusion on lower cervical facet joint fracture-dislocation. J Korean Orthop Assoc. 1997. 32:1078–1084.
19. Song KJ, Lee KB. Posterior reduction/fusion followed by anterior decompression/fusion of unreduced bilateral facet fracture-dislocation in the lower cervical trauma. Neurosurg Q. 2008. 18:109–114.
 XML Download
XML Download