

 PDF
PDF ePub
ePub Citation
Citation Print
Print


Abstract
Slippage of the upper femoral epiphysis can occur in association with endocrine disorder. A 14-year-old male patient, who complained of pain on multiple joints including both hips, was diagnosed with bilateral slipped femoral epiphysis due to primary hyperparathyroidism. At a single operation, the epiphyses were pinned-in situ, and the tumor was removed. After parathyroidectomy, the calcium and the parathyroid hormone levels promptly resolved. The pinning-in situ of both femoral heads was done for the purpose of preventing further displacement of the femoral epiphyses, and we aimed for epiphysiodesis. The permanent biopsy of the tumor was parathyroid adenoma. The physes of both femoral heads were closed and the widened physes of both distal tibias resolved postoperatively.
Figures and Tables

Fig. 2
(A) Right ankle anteroposterior radiograph showing widening of distal tibial epiphyseal plate. (B) The epiphyseal plate of right distal tibia narrowed at postoperatively nine months later.

Fig. 3
The axial image of pelvic bone computerized tomograph showing widening of both femoral epiphyseal plate and mild posterior migration of both femoral epiphyses.
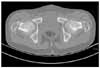


Fig. 6
The pins in both femoral head were removed at postoperatively nine months later. And the follow-up radiograph showing completely closing femoral capital epiphyseal plates.

Fig. 7
(A) The subperiosteal resorptions of phalanges were shown preoperatively. (B) The subperiosteal resorption of phalanges were reduced after operation.



References
1. Mann DC, Weddington J, Richton S. Hormonal studies in patients with slipped capital femoral epiphysis without evidence of endocrinopathy. J Pediatr Orthop. 1988. 8:543–545.

2. Well D, King JD, Roe TF, Kaufman FR. Review of slipped capital femoral epiphysis associated with endocrine disease. J Pediatr Orthop. 1993. 13:610–614.
3. Moorefield WG Jr, Urbaniak JR, Ogden WS, Frank JL. Acquired hypothyroidism and slipped capital femoral epiphysis, Report of three case. J bone joint Surg Am. 1976. 58:705–708.
4. Qadan L, Al-Quaimi M, Ahmad A. Slipped capital epiphysis associated with primary hyperparathyroidism and severe hypercalcemia. Clin Pediatr (Phila). 2003. 42:439–441.
5. Krempien B, Mehls O, Ritz E. Morphological studies on pathogenesis of epiphyseal slipping in uremic children. Virchows Arch A Pathol Anat Histol. 1974. 362:129–143.
6. Oppenheim WL, Bowen RE, McDonough PW, Funahashi TT, Saluskry IB. Outcome of slipped capital femoral epiphysis in renal osteodystrophy. Journal of Pediatric Orthopaedics. 2003. 23:169–174.
7. Bone LB, Roach JW, Ward WT, Worthen HG. Slipped capital femoral epiphysis associated with hyperparathyroidism. J Pediatr Orthop. 1985. 5:589–592.
8. Khiari K, Cherif L, Ben Abdalah N, et al. Slipped capital femoral epiphysis associated with hyperparathyroidism. A case report. Ann Med Interne (Paris). 2003. 154:544–546.
9. Yang WE, Shih CH, Wang KC, Jeng LB. Slipped capital femoral epiphyses in a patient with primary hyperparathyroidism. J Formos Med Assoc. 1997. 96:549–552.
10. Kinoshita J, Kaneda K, Matsuno T, Hosokawa Y, Nagashio R. Slipped capital femoral epiphysis associated with hyperparathyroidism. A case report. Int Orthop. 1995. 19:245–247.
 XML Download
XML Download