

 PDF
PDF ePub
ePub Citation
Citation Print
Print


Abstract
Purpose
We wanted to evaluate the effectiveness of posterolateral approach for open reduction and internal fixation of posterior malleolar fragment with trimalleolar fracture of ankle joint.
Materials and Methods
There were 27 cases of trimalleolar fracture in our hospital from Jan. 2005 to Dec. 2007. We investigated 10 patients who underwent operation with the posterolateral approach. The mean follow up period was 20 (6-36) months. Preoperative posterior malleolar fragment involved above 25% of articular surface in 10 cases and displaced more than 2 mm in 4 cases. We analyzed the radiologic type of posterior malleolar fragments and complications, and evaluated the AOFAS score.
Figures and Tables
Fig. 1
Posterolateral approach. (A) The longitudinal incision is placed just medial to the posterior border of the fibula. (B) Retracting the peroneal tendons medially gives access to the posterior aspect of the lateral malleolus. (C) View of the posterior fragment in the interval between the peroneal tendons and the flexor hallucis longus. (D) Posterior fragment was reduced and fixed with 1 or 2 of 4.0 mm cannulated screw.

Fig. 2
Transverse computed tomographic scan at the level of the tibial plafond showing posterolateral fragment of the posterior malleolus. We measured the area of the posterior malleolar fragment and the remaining cross-sectional area of the tibia.

Fig. 3
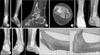
(A, B) Preoperative anteroposterior and lateral radiograph of the left ankle of a sixty-four-year-old man who vehicle accident, revealing an supination-external rotation injury and Weber B trimalleolar fracture with posterior malleolar fragment of 32% joint surface involved. He has a osteoporosis of T-score -3.8. (C, D) There is postoperative radiograph. (E, F) Radiograph made three months postoperatively, showing complete bony union.

Fig. 4
(A, B) Preoperative anteroposterior and lateral radiograph of the left ankle of a sixty-one-year-old man who slip down, revealing an supination-external rotation injury and Weber B trimalleolar fracture with posterior malleolar fragment of 25% joint surface involved. (C, D) Preoperative CT of the sagittal and axial view. It has posterolateral fragment. (E) There is postoperative radiograph. (F, G) Radiograph made six months postoperatively showing complete bone union. (H, I) Normal ankle joint motion of twelve months postoperatively.


References
1. Nugent JF, Gale BD. Isolated posterior malleolar ankle fractures. J Foot Surg. 1990. 29:80–83.
2. Haraguchi N, Haruyama H, Toga H, Kato F. Pathoanatomy of posterior malleolar fractures of the ankle. J Bone Joint Surg Am. 2006. 88:1085–1092.

3. Jaskulka RA, Ittner G, Schedl R. Fractures of the posterior tibial margin: their role in the prognosis of malleolar fractures. J Trauma. 1989. 29:1565–1570.
4. McDaniel WJ, Wilson FC. Trimalleolar fractures of the ankle. An end result stydy. Clin Orthop Relat Res. 1977. (122):37–45.
5. Talbot M, Steenblock TR, Cole PA. Posterolateral approach for open reduction and internal fixation of trimalleolar ankle fractures. Can J Surg. 2005. 48:487–490.
6. Carr J. Browner B, Jupiter J, Levine A, Trafton P, editors. Skeletal trauma: basoc science, management and reconstruction. 2003. Philadelphia: Elsevier Science;371–401.
7. Marsh JL, Saltzman C. Bucholz R, Heckman J, editors. Rockwood and Green's fractures in adults. 2001. Philadelphia: Lippincott, Williams & Wilkins;2001–2090.
8. Miller AJ. Posterior malleolar fractures. J Bone Joint Surg Br. 1974. 56:508–512.
9. Heim UF. Trimalleolar fractures: late results after fixation of the posterior fragment. Orthopedics. 1989. 12:1053–1059.
10. Kitaoka HB, Alexander IJ, Adelaar RS, Nunley JA, Myerson MS, Sanders M. Clinical rating systems for the ankle-hindfoot, midfoot, hallux, and lesser toes. Foot Ankle Int. 1994. 15:349–353.
11. Cooper A. A treatise on dislocations and on fractures of the joints: fractures of the neck of the thigh-bone. 1823. Clin Orthop Relat Res. 2007. 458:6–7.
12. Cotton FJ. A new type of ankle fracture. JAMA. 1915. 64:318–321.
13. Henderson MS. Trimalleolar fracture of the ankle. Surg Clin North AM. 1932. 12:867–872.
14. Burwell HN, Chanley AD. The treatment of displaced fractures at the ankle by rigid internal fixation and early joint movement. J Bone Joint Surg Br. 1965. 47:634–660.
15. Dickson FJ. Posterior marginal fracture of the tibia. Surg Gynecol Obstet. 1933. 56:525–528.
16. Dieterle J. The use of kirschner wires in maintaining reduction of fracture dislocation of the ankle joint: a report of two cases. J Bone Joint Surg Am. 1935. 17:990–995.
17. Broos PLO, Bisschop APG. Operative treatment of ankle fractures in adults: correlation between types of fracture and final results. Injury. 1991. 22:403–406.
18. van Laarhoven CJHM. Fractures of the ankle joint: Retrospective and prospective studies on the (long-term) results of protocolled treatment. 1994. Utrecht, The Netherlands: Academisch Ziekenhuis;112–118.
19. McLaughlin HI. Trauma. 1960. Philadelphia: WS Saunders Co;357.
20. Sachs W, Kanat IO, McLaughlin E, Burns DE. A surgical approach to a displaced ankle fracture. J Foot Surg. 1984. 23:302–307.
21. Jergeson F. Open reduction of fractures and dislocation of the ankle. Am J Surg. 1959. 98:136.
22. Henry AK. Extensile Exposure. 1973. Endinburgh: Churchill Livingstone.
23. Jeong HJ, Kim KC, Chung SW. Treatment of the posterior malleolar fracture. J Korean Fracture Soc. 1998. 11:924–931.
24. Kim SJ, Choi IY, Ahn TK. A clinical study of the trimalleolar fractures of the ankle. J Korean Fracture Soc. 1989. 2:145–154.
 XML Download
XML Download