

 PDF
PDF ePub
ePub Citation
Citation Print
Print


INTRODUCTION
Many studies have shown that the development of ankle arthritis is the result of a varienty of conditions, including primary osteoarthritis, post-traumatic osteoarthritis following the fracture or sprain, gouty osteoarthritis and rheumatic osteoarthritis14,16). Although non-surgical treatment may be successful in early arthritis, progressed arthritis requires surgical treatments such as a corrective osteotomy, ankle arthrodesis, or distraction arthroplasty using an external fixator or ankle joint arthroplasty.
Currently, the standard surgical treatment option is ankle arthrodesis5). However, total ankle arthroplasty has been considered because the long-term follow up has revealed potential shortcomings of ankle arthrodesis. Despite the increasing failure rates, the interest in total ankle arthroplasty has been renewed because ankle arthrodesis causes degenerative arthritis in the adjacent articulations and a limited range of motion in the latter stage. Although many surgeons believed in early days that the results of total ankle arthroplasty would be encouraging, several shortcomings have been reported including limited tolerance, low patient satisfaction and high complication rates. Many second-generation implants have been introduced as a result of the disadvantages of first-generation implants, among which Agility (Depuy, Warsaw, Indiana) is a prototypical design. There are few reports on the results of total ankle replacement using the Agility total ankle prosthesis in Korea whereas are many are available in other countries. Therefore, we report the short-term results of total ankle arthroplasty using the Agility prosthesis in patients with ankle osteoarthritis who did not respond to conservative management.
MATERIALS AND METHODS
1. Materials
This study reviewed the results of total ankle arthroplasty using the Agility prosthesis, which were performed between May, 2003 and May, 2004, in 10 patients (10 ankles, two males and eight females) suffering from ankle osteoarthritis despite medication, physical therapy, orthosis application and strengthening exercises over a 6 month period. All patients had a minimum postoperative follow up period of 2 years. The average age was 51.8 (range 41 to 67) years and the average follow up was 30.3 (range 24 to 36) months. The preoperative diagnoses were rheumatoid arthritis (3 ankles), primary osteoarthritis (3 ankles) and posttraumatic arthritis following an ankle fracture (4 ankles). All the procedures were performed by a single surgeon. Both the clinical and radiological results were reviewed at the postoperative 6 weeks, 3 months, 6 months, one year, then annually until the most recent follow up.
2. Methods
The clinical evaluation included the ankle range of motion, walking pain (VAS score) and the American Orthopaedic Foot and Ankle Society (AOFAS) ankle score6) at the most recent follow up. The overall range of motion was obtained using the method proposed by Coetzee et al3), who measured the angle formed between a line drawn from the superior horizontal plane of the tibial component to the inferior horizontal plane of the talar component and then the tibio-talar and the midfoot range of motion separately using a line extending from the axis of the first metatarsal. In addition, the patients were asked whether they were satisfied (excellent, good, fair, poor) with the outcome and if they would choose to undergo the procedure again. They were also asked if they used the orthosis. Weight bearing radiographs, consisting of anteroposterior, lateral, and mortice views as well as the lateral views of the ankle at maximal flexion and extension were reviewed at each follow up. In addition, the evidence of syndesmosis union, loosening and migration of the prosthesis, osteolysis, and posttraumatic hindfoot arthritis were also examined. The syndesmosis was examined for any evidence of union defined as bony trabeculation across the union site, and was defined as either union (in less than 6 months), delayed union(in more than 6 months), or nonunion (lack of union at the time of most recent follow up)11). Subsidence was measured using the relationship between the position of the component in a parallel plane and the sclerotic line near the osteotomy site8). The MML (medial malleolar line: the distance between the position of talar component in parallel plane and the tip of medial malleolus) was also measured11). Angular migration of a component was defined as evidence of a minimum of 5° shifts in the anteroposterior and lateral views, according to the protocol outlined by Saltzman et al11).
3. Surgical Techniques
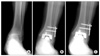
The preoperative evaluations including the size of implant and the extent of the osteotomy, were determined using plain radiographs. After spinal anesthesia, a sandbag was placed on the operating table under the hip involved in order to help maintain the ankle in the neutral position with the patient in the supine position. Initially, the external fixator was positioned over the tibia, the neck of the talus, and calcaneus, followed by traction of approximately 5 mm to 7 mm. The alignment of the ankle joint was then checked to determine if it was acceptable. The anterior surgical approach, using the interval between the anterior tibial tendon and the extensor hallucis longus tendon, was used to expose the ankle joint and place the Zig at the appropriate site so that the distal tibia and talar dome were resected approximately 4 to 5 mm and 5 to 6 mm, respectively. The implant was inserted and the soft tissues around the syndesmosis were debrided. A bone graft was performed with the remaining cancellous bones, and the syndesmosis was then fixed using two screws inserted percutaneously (Fig. 1). After skin closure, a short leg cast was applied. Wound care and swelling were managed for several days. This was followed by an additional 6 weeks of protected weight bearing in a short leg cast. Range of motion exercises and rehabilitation were initiated once the short leg cast had been removed.
RESULTS
1. Clinical Results
The mean preoperative and postoperative AOFAS ankle scores were 38.2 (range 14 to 52) and 73.8 (range 61 to 85), respectively, demonstrating significant improvement. The waking pain at the final follow up improved to an average of 2.8 (range 1 to 5), compared with 8.9 (range 8 to 10) before surgery. The mean ankle range of motion decreased slightly by 10° (range 0° to 25°) and 23% (range 0 to 50%) at the final follow up (Table 1). Five patients required a cane to walk. Among a total of ten patients, eight, one and one reported satisfaction, good and dissatisfaction with the clinical outcomes of their surgery, respectively. Interestingly, the improvement in the level of ankle pain resulted in satisfactory outcome on three out of eight patients even though they required a cane to walk. Five patients stated that they would undergo total ankle arthroplasty again under similar circumstances.
2. Radiographic Results
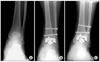
According to the final radiographic analysis, none of the ankles showed evidence of component migration in the transverse plane or evidence of sclerotic line changes. There was no subsidence of the components, as demonstrated by the lack of change in the MML. None of the components failed. Radiographic analysis showed a lucent line in all cases, which were, according to Pyevich and Saltzman et al11,13), three in Zone 6, one in Zone 1 to 6 and one in Zones 1, 5 and 6 on the anteroposterior radiographs. Lysis, involvement of only Zone 6, was noted in three ankles. One ankle with lysis showed progression, whereas the remaining subjects showed sclerosis at the last follow up radiographs (Fig. 2). Syndesmotic fusion was observed within 6 months in 5 ankles. Three ankles showed delayed union, taking longer than 6 months, but less than 10 months to unite. Two ankles were associated with nonunion on the syndesmosis. One patient was dissatisfied while the other was satisfied orgood. They all required a cane to walk and would not undergo a similar procedure under similar circumstances. Although there was a loss of sensation in the area innervated by the deep peroneal nerve in one patient, it returned normal at 6 months after surgery. One case was complicated by a lateral malleolar fracture, which was treated with cast immobilization and bony union was achieved (Fig. 3). Subtalar arthritis was observed in one ankle at 31 months after surgery (Table 2).
DISCUSSION
The Agility (Depuy, Warsaw, Indiana) and Scandinavian Total Ankle Replacement or STAR (Link Inc., Hamburg, Germany) are examples of prototypical second generation implants. The Agility ankle is especially popular in the USA and a two-component design that allows medial-lateral shift as well as axial rotation is commonly used because the polyethylene liner is firmly fixed to the tibial component. The syndesmotic fusion must be achieved for the Agility ankle, making it disadvantageous because nonunion of the syndesmosis is associated with the stability of the tibial component11). There are no standard parameters for measuring the ankle range of motion during the follow up after a total ankle replacement. Indeed, most studies have reported a mixture between the ankle and the midfoot range of motion2,7,17). The ankle range of motion reported by Pyevich et al11). was greater than in other reports, because they measured a mixture of the ankle and the midfoot range of motion. The method reported by Kitaoka and Patzer et al7). did not exclude the midfoot range of motion because the axis of the leg and foot using a goniometer on the lateral side was measured relatively. Therefore, Coetzee et al3). recommended a more objective and reliable method to measure the angle using the horizontal plane of a prosthesis. This led to a lower measured value than that measured in the above two studies. This shows that even a small change in the range of motion was exaggerated in most studies. At the final follow up, the average range of motion of ankle was 28° showing a mean 10° (range 0° to 25°) and 23% (range 0 to 50%) change compared with that measured before surgery. Another study reported a mean 36° change in the average range of motion after a mean follow up of 4.8 years11). The mean AOFAS score in this study at the last follow up was the average of 73.8 whereas Deland et al4). and Pyevich et al11). reported the average of 83.3 and 85, respectively. The difference in the AOFAS score was attributed to a higher union rate of syndesmosis.
According to Pyevich and Saltzman et al11,13), delayed union or nonunion of the distal syndesmosis is closely associated with the migration and stability of the tibial component and might result in an unsatisfactory clinical outcome. On the other hand, union of syndesmosis prevents subsidence of the tibial component from its further progression. They reported a nonunion rate of syndesmosis, and delayed union rate of 9% and 29%, respectively, after an average follow up of 4.8 years. In the other study, a 12% of nonunion rate was reported14). A literature review reported by Pomeroy and Barrow et al. showed a delayed union rate and nonunion rate of 29-38% and 9-18%, respectively1). The results from the present study, although a small group was involved, are considered to be similar to that of Pyevich and Saltzman et al. reported that two patients with nonunion showed fair and dissatisfaction. These patients required a cane to walk and said that they would not undergo the procedure again. Several studies including the injection of an autologous platelet concentrate1) and syndesmosis fixation using plate and multiple screws11) were carried out to promote a syndesmotic union. Using an autologous platelet concentrate, Barrow and Pomeroy et al1) reported union in all cases within 6 months. Pyevich and Saltzman et al11,13). reported that plate fixation of syndesmosis is a good method in that it not only it promotes union, but also it prevents and treats a fibular fracture. Therefore, it is currently favorable to use a plate and multiple screws for distal syndesmotic fixation. However in this study, distal syndesmotic fixation using a plate, with the aim of promoting union, resulted in nonunion because of screw loosening (Fig. 1). It is believed that this nonunion and loosening were attributed to the incomplete penetration of the screw into the medial tibial cortex and the syndesmotic instability by the tibial component upon weight bearing. Therefore, complete penetration of the screw into the medial tibia cortex will prevent the screws from loosening and promote union.
Pyevich et al. stated that periprosthetic radiographic lucency was always present in less than 2 years after surgery and ceased progression after several years. This was believed to result from the insufficient fixation of the component in the early stage. Osteolysis occurred frequently in the lateral side of the tibial component and occurred even more frequently when complicated by delayed union of the syndesmosis or nonunion. This was described as a result of bone absorbtion as a result of the shearing force produced between the remnant fibula and the lateral tibial component. In addition, of the end of progressive bone absorbtion could be indicated once sclerosis around the fibular margin was detected11).
Osteolysis in Zone 6 on the anteroposterior plain radiographs were reported to be closely related to the score of walking pain, whereas that in Zones 1 to 5 were associated with the subsidence of the tibial component11,13). Subsidence of the tibial component occurs less frequently than that of the talar component and the incidence of subsidence of talar components increases with time because there is no further progression of tibial subsidence is observed once syndesmotic fusion is completed11). Deland et al4). and Pyevich et al11). reported migration or a subsidence rate of the stem in 45% or 25.3%, respectively. However, the short-term follow up results of this study showed no subsidence or failure of the talar component. Degenerative changes to the adjacent joints are among the many complication encountered after ankle arthodesis. Many studies reported that hindfoot arthritis occurs in more than 50% and 100% after a follow up of 8 years and 20 years after ankle arthrodesis, respectively9,10,12). A total ankle replacement is associated with a much lower incidence of hindfoot arthritis than ankle arthrodesis.
However, Pyevich et al11). reported that the occurrence of hindfoot arthritis is not as rare as demonstrated by its less than 25% occurrence after a 7 year follow up. Deland et al4). and Salzman et al13). reported that the occurrence of hindfoot arthritis was 0% and 34%, respectively, at after a midterm follow up. In this study, one patient showed subtalar arthritis at the most recent follow up of 31 months and is currently under follow up.
The lower patient satisfaction rate in this study is believed to be associated with a lower rate of syndemosis union. Three techniques may improve the union rate of syndemosis. The first is a thorough debridement near the syndemosis and a sufficient autogenous bone graft. The second is the engagement of the far cortex in syndesmotic fixation using a plate. The third is an injection of an autologous platelet concentrate. Precise procedures and good planning will help achieve the better results.
CONCLUSION
The overall results of total ankle arthroplasty using the Agility prosthesis were favorable even though radiographic complications including nonunion of syndesmosis and periprosthetic osteolysis are often encountered. Despite of the small number of patients involved, syndesmotic nonunion was associated with the clinical results. However, long-term follow up will be neede to demonstrate osteolysis, loosening and subsidence of the talar component along with their clinical association.



 XML Download
XML Download