

 PDF
PDF ePub
ePub Citation
Citation Print
Print


Abstract
Purpose
To compare isometricity between the navigational and conventional technique during an anterior cruciate ligament (ACL) reconstruction before fixating the graft.
Materials and Methods
Twenty-three patients with an ACL insufficiency were enrolled in this study. After finishing the tibial tunnel preparation using a navigational technique, a femoral tunnel site was marked using either the navigational (Orthopilot®) or conventional (Arthrex® 5 mm off-set guide) technique. After passing the suture material attached to the guide pin through each femoral site, isometric tests were then performed using a specially designed device during full range of motion of the knee.
Results
An mean isometricity after the navigational and the conventional technique was 3.0 mm and 4.6 mm respectively. The isometricity after the navigational technique was significantly better than that after the conventional technique (p=0.000). The navigational isometric point was usually 0 to 5 mm anterior or antero-lateral to that at the point of the conventional technique. The mean distance between the tunnels by two techniques was 1.35 mm. There was a strong positive correlation between the difference in isometicity and the positional relationship of the femoral tunnel (r2=0.778, p=0.000).
Figures and Tables
 | Fig. 1Isometer consisting of a main frame, indicator and guide. Select the proper sized guide according to the size of tibial tunnel, indicator with regular tension during knee ROM, indicates scale drawn on main frame, scale differences imply isometricity. Measure scale differences by knee flexion & extension, and maximum difference is calculated in mm as isometricity.
|
 | Fig. 2Tibial and femoral passive transmitter is fixed securely. 4 balls located in transmitter reflect infrared rays. Reflected infrared rays from the generator were detected by camera in main system.
|
 | Fig. 3Tibial tunneling was done by navigational technique. (A) This is a tibial tunneling guide of navigational technique. (B) It showed the information indicated by tibial guide. This tibial tunnel was located in 20 degrees in coronal plane, 55 degrees in sagital plane, 8 mm anterior to PCL anterior edge, and 48% in medial tibial plateau.
|
 | Fig. 4Femoral tunneling was done by conventional technique with Arthrex® 5 mm off-set manual guide. Femoral tunneling was made toward 10 : 30 or 1 : 30 O'clock.
|
 | Fig. 5Fixation the guide attached by Ethibond® #5 through femoral cortex. Femoral side of Ethibond® #5 was firmly fixed to ACL attach site, act like reconstructed ACL at same location during the knee ROM. The length change was equal to isometricity of reconstructed ACL.
|
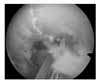
 | Fig. 6Isometricity was measured under knee ROM exercise. Pass the other end of Ethibond® #5 through tibial tunnel, fixation the Ethibond® #5 by mosquito after equipment isometer through tibial tunnel. White arrow indicated isometer, inserted to the tibial tunnel.
|
 | Fig. 7(A) Femoral tunnel was made by navigational technique. The appropriate isometric points by navigational technique is more antero-lateral than conventional technique. (B) Isometricity is 3 mm, and 1 : 30 O'clock position, 9 mm anterior to over the top position.
|
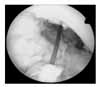
 | Fig. 8Positional relationship was measured by arthroscopy with a probe. (A) Black arrow indicats femoral tunnel by conventional technique and white arrow indicats femoral tunnel by navigational technique. Femoral tunnel by navigation technique was located more anterolateral position than by conventional technique, and difference between two tunneling was about 2 mm. (B) Femoral tunnel by navigation technique was located more anterior position than by conventional technique.
|





References
1. Aglietti P, Buzzi R, Menchetti P, Giron F. Arthroscopically assisted semitendinosus and gracillis tendon graft in reconstruction for acute anterior cruciate ligament injuries in athletes. Am J Sports Med. 1996. 24:726–731.
2. Alietti P, Buzzi Rm, D'Andria S, Zacchrott G. Long-term study of anterior cruciate ligament reconstruction for chronic insatbility using the central one-third patellar tendon and a lateral extraarticular tenodesis. Am J Sports Med. 1992. 20:38–45.
3. Allen CR, Griffin JR, Harner CD. Revision anterior cruciate ligament reconstruction. Orthop Clin North Am. 2003. 34:79–98.

4. Bealle D, Johnson DL. Technical pitfalls of anterior cruciate ligament surgery. Clin Sports Med. 1999. 18:831–845.
5. Buzzi R, Zaccherotti G, Giron F, Aglietti P. The relationship between the intercondylar roof and the tibial plateau with the knee in extension: relevance for tibial tunnel placement in anterior cruciate ligament reconstruction. Arthroscopy. 1999. 15:625–631.
6. Chouliaras V, Ristanis S, Moraiti C, Stergiou N, Georgoulis AD. Effectiveness of reconstruction of the anterior cruciate ligament with quadrupled hamstrings and bone-patellar tendon-bone autografts: an in vivo study comparing tibial internal-external rotation. Am J Sports Med. 2007. 35:189–196.
7. Daniel DM. Daniel DM, Akeson WH, O'Connor JJ, editors. Knee ligaments: structure, function, injury and repair. Principle of knee ligament surgery. 1990. New York: Raven Press;11–29.
8. Flemming BC, Beynnon BD, Nichols CE, Renström PA, Johnson RJ, Pope MH. An in-vivo comparison between intraoperative isometric measurement and local elongation of the graft after reconstruction of the anterior cruciate ligament. J Bone Joint Surg Am. 1994. 76:511–519.
9. Flemming BC, Beynnon BD, Johnson RJ, McLeod WD, Pope MH. Isometric versus tension measurements. A comparison for the reconstruction of the anterior cruciate ligament. Am J Sports Med. 1993. 21:82–88.
10. Gillquist J, Good L. Load and length changes in an artificial ligament substitute. 10 cases of anterior cruciate ligament reconstruction. Acta Orthop Scand. 1993. 64:575–579.
11. Graf B. Jackson DW, editor. Isometric placement of substitutes for the anterior cruciate ligament. The anterior crutiate deficient knee. New concepts in ligament repair. 1987. St. Louis: C.V. Mosby;102–113.
12. Graft B, Uhr F. Complications of intra-articular anterior cruciate reconstruction. Clin Sports Med. 1988. 7:835–848.
13. Graft BK, Rothenberg M, Vanderby R. Anterior cruciate ligament reconstruction with patellar tendon. An ex vivo study of wear-related damage and failure at the femoral tunnel. Am J Sprots Med. 1994. 22:131–135.
14. Hame SL, Markolf KL, Hunter DM, Oakes DA, Zoric B. Effects of notchplasty and femoral tunnel position on excursion patterns of an anterior cruciate ligament graft. Arthroplasty. 2003. 19:340–345.
15. Hart R, Krejzia J, Sváb P, Kocis J, Stipeák V. Outcomes after conventional versus computer navigated anterior cruciate ligament reconstruction. Arthroscopy. 2008. 24:569–578.
16. Hefzy MS, Grood ES, Noyes FR. Factors affecting the region of most isometric femoral attachments. Part II: The anterior cruciate ligament. Am J Sports Med. 1989. 17:208–216.
17. Howell SM, Wallace MP, Hull ML, Deutsch ML. Evaluation of the single-incision arthroscopic technique for anterior cruciate ligament replacement: a study of tibial tunnel placement, intraoperative graft tension, and stability. Am J Sports Med. 1999. 27:284–293.
18. Kenamori A, Woo SL, Ma CB, et al. The forces in the anterior cruciate ligament and knee kinematics during a simulated pivot shift test: a human cadaveric study using robotic technology. Arthroscopy. 2000. 16:633–639.
19. Koh JL. Navigation and ACL reconstruction. Presented at the 25th Annual Meeting of the Arthroscopy Association of North America. 2006. May. Hollywood. FL.
20. Loh JC, Fukuda Y, Tsuda E, Steadman RJ, Fu FH, Woo SL. Knee stability and graft function following anterior cruciate ligament reconstruction: comparison between 11 o'clock and 10 o'clock femoral tunnel placement. 2002 Richard O'Connor Award paper. Arthroscopy. 2003. 19:297–304.
21. Muneta T, Sekiya I, Yagishita K, Ogiuchi T, Yamamoto H, Shinomiya K. Two-bundle reconstruction of the anterior cruciate ligament using semitendinosus tendon with endobuttons: operative technique and preliminary results. Arthroscopy. 1999. 15:618–624.
22. O'Briend WR. Isometric placement of anterior cruciate ligament substitutes. . Oper Tech Orthop. 1992. 2:49–54.
23. O'Meara RP, O'Briend WR, Henning CE. Anterior cruciate ligament reconstruction stability with continuous passive motion: The role of isometric graft placement. Clin Orthop Relat Res. 1992. 277:201–209.
24. Penner DA, Daniel DM, Wood P, Mirshra D. An in-vitro study of anterior cruciate ligament graft placement and isometry. Am J Sports Med. 1988. 16:238–243.
25. Schutzer SF, Christen S, Jakob RP. Further observations of the isometricity of the anterior cruciate ligament. An anatomic study using a 6 mm diameter replacement. Clin Orthopn Relat Res. 1989. 242:247–255.
26. Scopp JM, Jasper LE, Belkoff SM, Moorman CT 3rd. The effect of oblique femoral tunnel placement on rotational constraint of the knee reconstructed using patellar tendon autografts. Arthroscopy. 2004. 20:294–299.
27. Seon JK, Park SJ, Lee KB, Yoon TR, Seo HY, Song EK. Stability comparison of anterior cruciate ligament between double- and single-bundle reconstructions. Int Orthop. 2009. 33:425–429.
28. Sidles JA, Larson RV, Garbini JL, Downey DJ, Matsen FA 3rd. Ligament length relationships in the moving knee. J Orthop Res. 1988. 6:593–610.
29. Sommer C, Friederich NF, Muller W. Improperly placed anterior cruciate ligament grafts: correlation between radiological parameters and clinical results. Knee Surg Sports Traumatol Arthrosc. 2000. 8:207–213.
30. Woo SL, Kanamori A, Zeminski J, Yagi M, Papageorgiou C, Fu FH. The effectiveness of reconstruction of the anterior cruciate ligament with hamstrings and patellar tendon. A cadaveric study comparing anterior tibial and rotational loads. J Bone Joint Surg Am. 2002. 84:907–914.
31. Yagi M, Wong EK, Kanamori A, Debski RE, Fu FH, Woo SL. The biomechanical analysis of anatomical ACL reconstruction. Am J Sports Med. 2002. 30:660–666.
32. Yasuda K, Kondo E, Ichiyama H, Tanabe Y, Tohyama H. Clinical evaluation of anatomic double-bundle anterior cruciate ligament reconstruction procedure using hamstring tendon grafts: comparisons among 3 different procedures. Arthroscopy. 2006. 22:240–251.
 XML Download
XML Download