

 PDF
PDF ePub
ePub Citation
Citation Print
Print


Abstract
Purpose
Several treatment options have been reported for post-traumatic kyphosis (PTK) and neurologically compromised osteoporotic fractures. However, there is no ideal surgical procedure. This study evaluated the effectiveness of posterolateral decompression and anterior support with a titanium mesh in PTK by posterior surgery.
Materials and Methods
Seventeen patients with PTK and neurologically compromised osteoporotic fractures underwent a single posterior approach. During posterior decompression, a titanium mesh was inserted through the posterior approach after a transpedicular intracorporeal corpectomy. Complications, operating time and blood loss were noted, and radiographic studies and neurological status were evaluated before surgery, after surgery, and at final follow-up.
Results
The mean kyphosis was 35±9.7° (range; 17-58°) before surgery, 3.2±1.8° after surgery (correction; 90.5%) and 5.5±3.2° at the final follow-up (correction; 85.5%). There was 29.6° correction of the kyphosis with a 6% loss of correction. Postoperative neurological improvement using the Frankel classification was demonstrated in all patients. There was no new onset or progressive neurological deterioration, additional surgery or extrusion of mesh. Three complications were encountered: one care each of pneumonia, prolonged ventilator support and distal adjacent vertebral fracture.
Figures and Tables
Fig. 1
77-year-old female sustained a L1 compression fracture 1 year earlier. She presented with post-traumatic kyphosis and neurological compromise that had developed 3 months earlier. (A) Preoperative radiographs show a burst out and kyphotic deformity on the standing radiographs and a vacuum cleft of L1 on the recumbent radiograph. Preoperative neurological deficit was Frankel grade C. (B) T2-weighted sagittal MR image shows retropulsed bony fragments into the spinal canal and avascular necrosis on the T12 and L1 body. (C) The axial MR image shows compression of the spinal cord at the L1 level.

Fig. 2
(A) Postoperative radiographs show that the kyphosis was corrected to 0°. (B) The postoperative radiographs taken three years after surgery show that the reconstructed portion of the spine is stable with the correction of kyphosis being maintained.
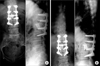
Fig. 3
64-year-old female was injured by slip down and sustained a L1 compression fracture 2 months before presentation. Before presentation at our facility, she was treated with kyphoplasty and presented to our institution with severe back pain and paraparesis that developed one month after kyphoplasty. (A) Post-trauma lateral radiograph. (B) Radiograph taken 2 weeks after the injury shows a collapse of the vertebral body. (C) Immediate lateral radiograph after kyphoplasty. (D) Preoperative lateral radiograph shows the collapsed vertebral body at L1 with 32° of kyphosis. The patient had Frankel grade D before surgery. (E) The preoperative MR images show the avascular necrosis of the L1 body, retropulsed bony fragments into the spinal canal and neural compression at the level of L1.

Fig. 4
(A) Intraoperative findings; working space made by pedicle subtraction (empty arrow), extraction of cement mass through the space (short arrow), covering of interlaminar defect with splitted interspinous process following transpedicular intracoporeal corpectomy and rods fixation (long arrow) and posterior fusion (dotted arrow). (B) Cement mass from vertebral body. (C) 3D-reconstruction CT sacns show the reconstructed portion of the spine is stable and the correction of kyphosis is well maintained. (D) Postoperative radiographs tatken sixteen months after the surgery show that kyphosis was corrected to 0°.


References
1. Alanay A, Pekmezci M, Karaeminogullari O, et al. Radiographic measurement of the sagittal plane deformity in patients with osteoporotic spinal fractures evaluation of intrinsic error. Eur Spine J. 2007. 16:2126–2132.

2. Barr JD, Barr MS, Lemley TJ, McCann RM. Percutaneous vertebroplasty for pain relief and spinal stabilization. Spine. 2000. 25:923–928.
3. Bohlman HH, Freehafer A, Dejak J. The results of treatment of acute injuries of the upper thoracic spine with paralysis. J Bone Joint Surg Am. 1985. 67:360–369.
4. Bradford DS, McBride GG. Surgical management of thoracolumbar spine fractures with incomplete neurologic deficits. Clin Orthop Relat Res. 1987. 218:201–216.
5. Capener N. The evolution of lateral rhachotomy. J Bone Joint Surg Br. 1954. 36:173–179.
6. Eysel P, Schwitalle M, Oberstein A, Rompe JD, Hopf C, Küllmer K. Preoperative estimation of screw fixation strength in vertebral bodies. Spine. 1998. 23:174–180.
7. Gertzbein SD, Harris MB. Wedge osteotomy for the correction of post-traumatic kyphosis. A new technique and a report of three cases. Spine. 1992. 17:374–379.
8. Heinig CF. Luque E, editor. Eggshell procedure. Segmental spinal instrumentation. 1984. New Jersey: Slack;221–234.
9. Holdsworth FW, Hardy A. Early treatment of paraplegia from fractures of the thoraco-lumbar spine. J Bone Joint Surg Br. 1953. 35:540–550.
10. Jensen ME, Evans AJ, Mathis JM, Kallmes DF, Cloft HJ, Dion JE. Percutaneous polymethylmethacrylate vertebroplasty in the treatment of osteoporotic vertebral body compression fractures: technical aspects. AJNR Am J Neuroradiol. 1997. 18:1897–1904.
11. Jodoin A, Gillet P, Dupuis PR, Maurais G. Surgical treatment of post-traumatic kyphosis: a report of 16 cases. Can J Surg. 1989. 32:36–42.
12. Kaneda K, Asano S, Hashimoto T, Satoh S, Fujiya M. The treatment of osteoporotic-posttraumatic vertebral collapse using the Kaneda device and a bioactive ceramic vertebral prosthesis. Spine. 1992. 17(8 Suppl):S295–S303.
13. Kawahara N, Tomita K, Baba H, Kobayashi T, Fujita T, Murakami H. Closing-opening wedge osteotomy to correct angular kyphotic deformity by a single posterior approach. Spine. 2001. 26:391–402.
14. Kim KT, Suk KS, Kim JM, Lee SH. Delayed vertebral collapse with neurological deficits secondary to osteoporosis. Int Orthop. 2003. 27:65–69.
15. Kostuik JP. Anterior Kostuik-Harrington distraction systems for the treatment of kyphotic deformities. Spine. 1990. 15:169–180.
16. Kostuik JP, Matsusaki H. Anterior stabilization, instrumentation, and decompression for post-traumatic kyphosis. Spine. 1989. 14:379–386.
17. Kumpan W, Salomonowitz E, Seidl G, Wittich GR. The intravertebral vacuum phenomenon. Skeletal Radiol. 1986. 15:444–447.
18. Lee TT, Alameda GJ, Gromelski EB, Green BA. Outcome after surgical treatment of progressive posttraumatic cystic myelopathy. J Neurosurg. 2000. 92(2 Suppl):S149–S154.
19. Lehmer SM, Keppler L, Biscup RS, Enker P, Miller SD, Steffee AD. Posterior transvertebral osteotomy for adult thoracolumbar kyphosis. Spine. 1994. 19:2060–2067.
20. Leidholt JD, Young JJ, Hahn HR, Jackson RE, Gamble WE, Miles JS. Evaluation of late spinal deformities with fracture-dislocations of the dorsal and lumbar spine in paraplegics. Paraplegia. 1969. 7:16–28.
21. Malcolm BW, Bradford DS, Winter RB, Chou SN. Post-traumatic kyphosis. A review of forty-eight surgically treated patients. J Bone Joint Surg Am. 1981. 63:891–899.
22. McAfee PC, Bohlman HH, Yuan HA. Anterior decompression of traumatic thoracolumbar fractures with incomplete neurological deficit using a retroperitoneal approach. J Bone Joint Surg Am. 1985. 67:89–104.
23. Murrey DB, Brigham CD, Kiebzak GM, Finger F, Chewning SJ. Transpedicular decompression and pedicle subtraction osteotomy (eggshell procedure): a retrospective review of 59 patients. Spine. 2002. 27:2338–2345.
24. Oner FC, van Gils AP, Faber JA, Dhert WJ, Verbout AJ. Some complications of common treatment schemes of thoracolumbar spine fractures can be predicted with magnetic resonance imaging: prospective study of 53 patients with 71 fractures. Spine. 2002. 27:629–636.
25. Roberson JR, Whitesides TE Jr. Surgical reconstruction of late post-traumatic thoracolumbar kyphosis. Spine. 1985. 10:307–312.
26. Roberts JB, Curtiss PH Jr. Stability of the thoracic and lumbar spine in traumatic paraplegia following fracture or fracture-dislocation. J Bone Joint Surg Am. 1970. 52:1115–1130.
27. Royle ND. The operative removal of an accessory vertebra. Med J Aust. 1928. 1:467.
28. Saita K, Hoshino Y, Kikkawa I, Nakamura H. Posterior spinal shortening for paraplegia after vertebral collapse caused by osteoporosis. Spine. 2000. 25:2832–2835.
29. Shikata J, Yamamuro T, Iida H, Shimizu K, Yoshikawa J. Surgical treatment for paraplegia resulting from vertebral fractures in senile osteoporosis. Spine. 1990. 15:485–489.
30. Shufflebarger HL, Clark CE. Thoracolumbar osteotomy for postsurgical sagittal imbalance. Spine. 1992. 17(8 Suppl):S287–S290.
31. Streitz W, Brown JC, Bonnett CA. Anterior fibular strut grafting in the treatment of kyphosis. Clin Orthop Relat Res. 1977. 128:140–148.
32. Suk SI, Kim JH, Lee SM, Chung ER, Lee JH. Anterior-posterior surgery versus posterior closing wedge osteotomy in posttraumatic kyphosis with neurologic compromised osteoporotic fracture. Spine. 2003. 28:2170–2175.
33. Sutherland CJ, Miller F, Wang GJ. Early progressive kyphosis following compression fractures. Two case reports from a series of "stable" thoracolumbar compression fractures. Clin Orthop Relat Res. 1983. 173:216–220.
34. Tanaka S, Kubota M, Fujimoto Y, Hayashi J, Nishikawa K. Conus medullaris syndrome secondary to an L1 burst fracture in osteoporosis. A case report. Spine. 1993. 18:2131–2134.
35. Vaccaro AR, Silber JS. Post-traumatic spinal deformity. Spine. 2001. 26(24 Suppl):S111–S118.
36. Wu SS, Hwa SY, Lin LC, Pai WM, Chen PQ, Au MK. Management of rigid post-traumatic kyphosis. Spine. 1996. 21:2260–2266.
 XML Download
XML Download