

 PDF
PDF ePub
ePub Citation
Citation Print
Print


Abstract
Purpose
To evaluate the results of physeal bar resection and free fat graft as a treatment method for partial epiphyseal closure.
Materials and Methods
Thirteen cases of partial epiphyseal closure (4 of the distal femur, 8 of the distal tibia and one of the distal radius) were subjected to physeal bar resection. All of the cases were caused by trauma. The physeal bar was central in 3 cases, peripheral in 9, and mixed (central-peripheral) in 1. Mean patient age at surgery was 10.7 years and mean follow-up period was 47 months. Final results were evaluated by a modified Williamson-Staheli classification.
Results
Results at final follow-up were as follows: 6 satisfactory (3 excellent and 3 good) and 7 unsatisfactory (5 fair and 2 poor). Satisfactory results according to location and region of the physeal bar were as follows: distal tibia, 5 of 8 cases; distal femur, 1 of 4; central, 1 of 3; peripheral, 4 of 9; and mixed, 1 of 1. When considered by areal extent, physeal bars occupying 30% or less of the bone's cross-sectional area showed satisfactory results in 5 of 7 cases, while in 6 cases with the physeal bar over 30%, 5 were unsatisfactory.
Figures and Tables
 | Fig. 1Diagrammatic representation of the physeal bar on A-P and lateral tomograms. With special care taken to keep its relative size and proportion, final cross section map was made by synthesis of physeal bar images from all tomographic levels (Carlson and Wenger method).
|
 | Fig. 2(A) Coronal image of the left ankle: note oblique orientation of the growth plate due to a medial growth plate injury. If the axial section does not include the whole growth plate due to the irregularity of the latter, it will not reflect the true extent of the physeal bar (upper line involves a lateral growth plate and lower line involves a medial growth plate). (B) Synthesis of physeal bars images from two consecutive axial views is required for accurate measurement of the extent of bar.
|
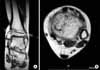
 | Fig. 3(A) Initial A-P radiograph of the left distal tibia of a 9 year and 3 month-old girl (5 months after growth plate injury) showing the epiphyseal bar. (B) CT of the growth plate shows the peripheral location of the bar. (C) Mapping by the method of Carlson and Wenger shows that the peripheral bar occupies 27% of the growth plate. (D) Postoperative A-P radiograph showing the screw that was placed as a marker to check growth after surgery. (E) A-P radiograph taken 24 months after surgery shows a good result: the marker has moved proximally as a result of longitudinal growth.
|
 | Fig. 4(A) Initial A-P and lateral radiographs of a 13 year and 8 month-old boy showing the epiphyseal bar formation following supracondylar fracture of the right distal femur. (B) T2-weighted coronal and sagittal MR images show the central physeal bar. (C) Mapping by the mothod of Carlson and Wenger shows that the physeal bar occupies 22% of the central area of the growth plate. (D) Intraoperative fluoroscopy image showing excision of the bar using a dental burr inserted through the metaphyseal window. (E) Postoperative radiographs (A-P and lateral views): a K-wire was used to fix the inserted autogenous fat graft in place, and also to serve as a marker to check further growth after surgery. (F) A-P radiograph taken 20 months after surgery showed 3 cm leg length discrepancy and a residual genu valgum of 7 degrees in the affected leg. The patient had a fair result. (G) An Ilizarov external fixator was applied to correct both problems. (H) A-P radiograph taken 24 months after surgery showed no leg length discrepancy. Deformity was corrected.
|



References
1. Bright RW. Operative correction of partial epiphyseal plate closure by osseous-bridge resection and silicone-rubber implant. An experimental study in dogs. J Bone Joint Surg Am. 1974. 56:655–664.
2. Bright RW. Partial growth arrest: identification, classification and results of treatment. Orthop Trans. 1982. 6:65–66.
3. Broughton NS, Dickens DR, Cole WG, Menelaus MB. Epiphyseolysis for partial growth plate arrest. Results after four years or at maturity. J Bone Joint Surg Br. 1989. 71:13–16.

4. Cady RB, Spadaro JA, Fitzgerald JA, Pinkes J, Albanese SA. The effects of fat interposition for central-physeal defects. A histologic study in rabbits. Clin Orthop Relat Res. 1992. 282:304–309.
5. Carlson WO, Wenger DR. A mapping method to prepare for surgical excision of partial physeal arrest. J Pediatr Orthop. 1984. 4:232–238.
6. Choi IH, Yoo WJ. Prognostic factors of physeal bar resection and fat graft interposition in the treatment of partial physeal arrest. J Korean Orthop Assoc. 1996. 31:649–658.
7. Hasler CC, Foster BK. Secondary tethers after physeal bar resection: a common source of failure? Clin Orthop Relat Res. 2002. 405:242–249.
8. Kasser JR. Physeal bar resections after growth arrest about the knee. Clin Orthop Relat Res. 1990. 255:68–74.
9. Khoshhal KI, Kiefer GN. Physeal bridge resection. J Am Acad Orthop Surg. 2005. 13:47–58.
10. Klassen RA, Peterson HA. Excision of physeal bars: the Mayo Clinic experience 1968-1978. Orthop Trans. 1982. 6:65.
11. Langenskiöld A, Heikel HV, Nevalainen T, Osterman K, Videman T. Regeneration of the growth plate. Acta Anat (Basel). 1989. 134:113–123.
12. Langenskiöld A. Surgical treatment of partial closure of the growth plate. J Pediatr Orthop. 1981. 1:3–11.
13. Langenskiöld A. Traumatic premature closure of the distal tibial epiphyseal plate. Acta Orthop Scand. 1967. 38:520–531.
14. Lee DY, Choi IH, Cung CY. An experience of bone bridge resection and free fat interposition for partial epiphyseal plate closure. J Korean Orthop Assoc. 1990. 25:187–196.
15. Mizuta T, Benson WM, Foster BK, Paterson DC, Morris LL. Statistical analysis of the incidence of physeal injuries. J Pediatr Orthop. 1987. 7:518–523.
16. Ogden JA. Ogden JA, editor. Management of growth mechanism injuries an arrest. Skeletal injury in the child. 2000. 3rd ed. New York: Springer-Verlag;209–242.
17. Ogden JA. The evaluation and treatment of partial physeal arrest. J Bone Joint Surg Am. 1987. 69:1297–1302.
18. Peterson HA. Partial growth plate arrest and its treatment. J Pediatr Orthop. 1984. 4:246–258.
19. Peterson HA, Madhok R, Benson JT, Ilstrup DM, Melton LJ 3rd. Physeal fractures: Part I. Epidemiology in Olmsted County, Minnesota, 1979-1988. J Pediatr Orthop. 1994. 14:423–430.
20. Vickers DW. Premature incomplete fusion of the growth plate: causes and treatment by resection (physolysis) in fifteen cases. Aust N Z J Surg. 1980. 50:393–401.
21. Williamson RV, Staheli LT. Partial physeal growth arrest: treatment by bridge resection and fat interposition. J Pediatr Orthop. 1990. 10:769–776.
 XML Download
XML Download