

 PDF
PDF ePub
ePub Citation
Citation Print
Print


Abstract
Purpose
In this retrospective study, we tried to find out potential prognostic factors that can be used to determine the optimal treatment for some conditions that are indicated for surgery like pathological fractures or epidural compression.
Materials and Methods
Between 1985 and 2003 we treated 78 patients with skeletal metastases. A multivariable analysis was conducted using the Cox proportional hazard model. The rates of survival were calculated by the Kaplan-Meier method.
Results
We identified four significant prognostic factors for survival: the site of the primary lesion, the presence of visceral or cerebral metastases, any previous chemotherapy and multiple skeletal metastases. With these factors, we could divide the patients into two prognostic groups: the good prognostic group satisfies more than two of the four significant factors and the poor prognostic group doesn't. For the good prognostic group, the average rates of survival at 6 months and a year were 95% and 28%, respectively, and those for the poor prognostic group were 28% (6 mo) and 13% (1 yr), respectively.
Conclusion
Each patient's life expectancy should be considered when we decide the surgical method for treating metastatic bone tumor. Patients with a very short life expectancy should probably be treated with a less invasive method but patients with a long life expectancy require aggressive surgery. If the life expectancy is estimated to be at least more than 2 month and 3-6 months for bony metastases to the extremity and spine respectively, then an aggressive surgical method should be chosen. With these practical prognostic factors, the life expectancy may be predicted more accurately and so the optimal surgical treatment can be selected more appropriately.
Figures and Tables
Fig. 1
This graph shows the Kaplan-Meier cumulative survival rates for the 78 patients. The overall survival rates were 68% for 6 months, 47% for 1 year, 35% for 2 years and 22% for 3 years.

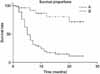
Fig. 2
This graph shows the Kaplan-Meier survival curves for the patients fo the good (A) and poor (B) prognostic group. The good prognostic group satisfies more than two of the four significant factors and the poor prognostic group doesn't. The rates of survival for these two groups are significantly different (log-rank test, p<0.0001).



References
1. Aaron AD. Treatment of metastatic adenocarcinoma of the pelvis and the extremities. J Bone Joint Surg Am. 1997. 79:917–932.
2. Atanasiu JP, Badatcheff F, Pidhorz L. Metastatic lesions of the cervical spine. A retrospective analysis of 20 cases. Spine. 1993. 18:1279–1284.

3. Bauer HC, Wedin R. Survival after surgery for spinal and extremity metastases. Prognostication in 241 patients. Acta Orthop Scand. 1995. 66:143–146.
4. Cox DR. Regression models and life tables. JR Stat Soc Br. 1972. 34:187–220.
5. Cybulski GR, Von Roenn KA, D'Angelo CM, DeWald RL. Luque rod stabilization for metastatic disease of the spine. Surg Neurol. 1987. 28:277–283.
6. DeWaId RL, Bridwell KH, Prodromes C, Rodts MF. Reconstructive spinal surgery as palliation for metastatic malignancies of the spine. Spine. 1985. 10:21–26.
7. Dürr HR, Maier M, Pfaler M, Baur A, Refior HJ. Surgical treatment of osseous metastases in patients with renal cell carcinoma. Clin Orthop Relat Res. 1999. 367:283–290.
8. Fidler MW. Anterior decompression and stabilization of metastatic spinal fractures. J Bone Joint Surg Br. 1986. 68:83–90.
9. Hansen BH, Keller J, Laitinen M, et al. The Scandinavian Sarcoma Group Skeletal Metastasis Register. Survival after surgery for bone metastases in the pelvis and extremities. Acta Orthop Scand. 2004. 75:Suppl. S11–S15.
10. Harrington KD. Anterior decompression and stabilization of the spine as a treatment for vertebral collapse and spinal cord compression from metastatic malignancy. Clin Orthop Relat Res. 1988. 223:177–197.
11. Harrington KD. Orthopaedic management of metastatic bone disease. 1988. 1st ed. Louis, etc: The CV Mosby Company;141–143.
12. Hipp JA, Springfield DS, Hayes WC. Predicting pathologic fracture risk in the management of metastatic bone defects. Clin Orthop Relat Res. 1995. 312:120–135.
13. Hosono N, Yonenobu K, Fuji T, Ebara S, Yamashita K, Ono K. Vertebral body replacement with a ceramic prosthesis for metatastic spinal tumors. Spine. 1995. 20:2454–2462.
14. Kaplan EL, Meier P. Nonparametric estimation for incomplete observation. J Am Stat Assoc. 1958. 53:457–481.
15. Lee HG, Lee SH, Baek KH, Lee CS. Surgical treatment of metastastic bone tumor in extremity. J Korean Bone & Joint Tumor Soc. 1995. 1:45–51.
16. Lodwick GS, Wilson AJ, Farrell C, Virtama P, Dittrich F. Determining growth rates of focal lesions of bone from radiographs. Radiology. 1980. 134:577–583.
17. Malchau H, Herberts P, Esler T, Garellick G, Söderman P. The Swedish Total Hip Replacement Reigster. J Bone Joint Surg Am. 2002. 84:Suppl 2. S2–S20.
18. Milch RA, Changus GW. Response of bone to tumor invasion. Cancer. 1956. 9:341–351.
19. Mirels H. Metastatic disease in long bones. A proposed scoring system for diagnosing impending pathologic fractures. Clin Orthop Relat Res. 1989. 249:256–264.
20. Rompe JD, Eysel P, Hopf C, Heine J. Metastatic instability at the proximal end of the femur. Comparison of endoprosthetic replacement and plate osteosynthesis. Arch Orthop Trauma Surg. 1994. 113:260–264.
21. Sherry MM, Greco FA, Johnson DH, Hainsworth JD. Breast cancer with skeletal metastases at initial diagnosis. Distinctive clinical characteristics and favorable prognosis. Cancer. 1986. 58:178–182.
22. Spiegel DA, Sampson JH, Richardson WJ, et al. Metastatic melanoma to the spine. Demographics, risk factors, and prognosis in 114 patients. Spine. 1995. 20:2141–2146.
23. Sundaresan N, Rothman A, Manhart K, Kelliher K. Surgery for solitary metastases of the spine: rationale and results of treatment. Spine. 2002. 27:1802–1806.
24. Teshima T, Chatani M, Inoue T, et al. Prognostic factors for patients with osseous metastasis: a multi-institutional prospective study. Strahlenther Onkol. 1990. 166:387–391.
25. Tokuhashi Y, Matsuzaki H, Toriyama S, Kawano H, Ohssaka S. Scoring system for preoperative evaluation of metastatic spine tumor prognosis. Spine. 1990. 15:1110–1113.
26. Tomita K, Kawahara N, Kobayashi T, Yoshida A, Murakami H, Akamaru T. Surgical strategy for spinal metastases. Spine. 2001. 26:298–306.
27. Ward WG, Holsenbeck S, Dorey FJ, Spang J, Howe D. Metastatic disease of the femur: surgical treatment. Clin Orthop Relat Res. 2003. 415:Suppl. S230–S244.
28. Weber KL, O'Connor MI. Operative treatment of long bone metastases: focus on the femur. Clin Orthop Relat Res. 2003. 415:Suppl. S276–S278.
29. Wedin R, Bauer HC, Rutqvist LE. Surgical treatment for skeletal breast cancer metastases: a population-based study of 641 patients. Cancer. 2001. 92:257–262.
30. Wise JJ, Fischgrund YS, Herkowitz HN, Montgomery D, Kurz LT. Complication, survival rates, and risk factors of surgery for metastatic disease of the spine. Spine. 1999. 24:1943–1951.
31. Yamashita K, Denno K, Ueda T, et al. Prognostic significance of bone metastases in patients with metastatic prostate cancer. Cancer. 1993. 71:1297–1302.
32. Yamashita K, Ueda T, Komatsubara Y, et al. Breast cancer with bone-only metastases. Visceral metastases-free rate in relation to anatomic distribution of bone metastases. Cancer. 1991. 68:634–637.
33. Yazawa Y, Frassica FJ, Chao EY, Pritchard DJ, Sim FH, Shives TC. Metastatic bone disease. A study of the surgical treatment of 166 pathologic humeral and femoral fractures. Clin Orthop Relat Res. 1990. 251:213–219.
 XML Download
XML Download