

 PDF
PDF ePub
ePub Citation
Citation Print
Print


INTRODUCTION
In children, fractures of the femoral shaft have been traditionally treated with immobilization in a spica cast, either immediately or after a period in traction. Recently, various treatments have been chosen according to the patient's age, associated injury, location of the fracture, degree of soft tissue injury, or the experience of the surgeon1,2,8,14).
In children, five years of age or younger, early closed reduction and the application of a spica cast is accepted as the ideal treatment for most diaphyseal femoral fractures. In skeletally matured adolescents older than 12 years, the use of firm internal fixation has become the standard of treatment. However, for children between ages 6 and 11, various methods including an early spica cast, external fixation, compression plating and intramedullary nailing with either rigid or flexible nails have been introduced. Recently, external fixation (EF) and flexible intramedullary nailing (FIN) have become the most widely used methods.
We report the treatment results as well as the advantages and disadvantages of 15 cases of FIN and 13 cases of EF for an isolated femoral shaft fracture in children aged between 6 and 11 years.
MATERIALS AND METHODS
This study involved 28 children with an isolated femoral shaft fracture between the ages of 6 and 11 years, who were treated either with EF or FIN between March, 1999 and February, 2004. Seventeen boys and 11 girls with a mean age was 8.6 years were followed-up for an average of 27.3 months (from 24 to 36 months). Eighteen cases were caused by traffic accidents, 6 cases were due to falls, and 4 cases were sports injuries. Fourteen cases were transverse fractures and 9 cases were oblique, and 5 cases were spiral fractures. Nineteen cases were midshaft fractures, 6 were proximal, and 3 cases were distal fractures.
We were unable to randomize the treatment methods. Instead, the choice of treatment of either EF or FIN was based on the preference of the 3 attending orthopedic surgeons. Fifteen children were treated with FIN using stainless steal 3.5 mm Ender nails, and 13 children were treated with EF (Dyna-Extor®, BK meditech Ltd, Korea). The operations were performed on a fracture table under general anesthesia with fluoroscopic control. For FIN, the Ender nail first was inserted on the lateral side 3 cm proximal from the distal epiphyseal plate and the tip of the nail came to rest immediately distal to the trochanteric apophysis. The opposite nail was inserted on the medial side of the cortex at the same level, and the tip pointed toward the calcar region of the femoral neck (Fig. 1). For EF, 2 pins were applied to each of the fragments. An end-to-end apposition was made on the transverse fractures, and 5 of angulation and bayonet apposition <1 cm was allowed for spiral and oblique fractures without a rotational deformity. Postoperative immobilization, either with splints or braces, was not performed. Partial weight bearing was allowed when the calluses had formed, and full weight bearing was allowed when 3/4 of the circumference of the fracture site was surrounded by calluses.
Bone union was defined as no pain on the fractures sites with circumferential calluses on more than 3/4 of the fracture site, the state of connection of the trabecular and the maturity of the callus. At this time for EF, the device was removed and a splint was applied for 2 weeks before weight bearing was allowed. For FIN, the Ender nails were removed 6 to 12 months (average 8.3 month) after surgery under general anesthesia and the patients were followed-up every 6 months.
Records of the time from injury to union, reduction failure, angular deformity, infection, and refracture were carefully made, and the end results were compared according to the limitation of knee motion, rotational malalignment, angular deformity, leg length discrepancy on the radiograph and limping.
RESULTS
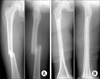
Bone union was achieved in all cases, and no child sustained a complication that was expected to cause a permanent disability. For FIN, union occurred at an average of 9.1 weeks (7-12 weeks). For EF, union was observed at an average of 11.2 weeks (9-14 weeks) with the exception of one case of metal breakage. In the FIN group, one lateral nail migrated distally and reinserted at 4 weeks but there were no complications such as infection, reduction loss, or bursitis on the nail insertion site. In the EF group, 3 patients had a pin site infection, which was treated with antibiotics and healed after removing the device at the time of union. One patient sustained a refracture 3 weeks after removing the external fixator and was treated with a compression plate (Fig. 2). One patient sustained metal failure at 8 weeks. The pin was removed, and a compression plate was applied. One patient had anteromedial angulation >10 on the follow-up. Therefore, a correction was made, and the device was removed at 14 weeks. The flexible intramedullary nail was removed at an average of 8.3 months (6-12 months) after surgery and the external fixators were removed after an average of 11.4 weeks (9-14 weeks).
On the last follow-up, no child had any limitations of hip or knee motion, or a limping gate. On the radiograph, no child had a shortening of the injured side. An average 4.2 mm (2-11 mm) and 3.8 mm (1-10 mm) leg length discrepancy was noticed in the FIN and EF groups, respectively. In addition, 2 children were treated with a compression plate due to complications had 8 mm, and 11 mm overgrowth respectively but were free of limping. There was no angular deformity >5 in the FIN Group but 2 children had 5-10 of anteromedial angulation the EF group. However, this had no observable effect on the final outcome.
DISCUSSION
Recently, for children aged between 6 to 11 years there has been a growing trend towards surgical treatment for isolated femoral shaft fractures, which is beneficial in shortening the time of knee, and hip immobilization and allowing early ambulation, which will have economic and sociopsychological effects on the children and their families2,4,14). Internal fixation with compression plates requires a wide dissection of the soft tissue and additional surgery for removal9). Rigid intramedullary nailing might cause trochanteric growth arrest and avascular necrosis of the femoral head. Therefore, EF and FIN are widely-used options for children between 6 to 11 years of age. In this study, femoral shaft fractures associated with head injuries, multiple fractures, or open fractures, which are general indications for surgery, were excluded, and only isolated femoral shaft fractures were examined.
EF involves no soft tissue dissection and leaves little scarring, and is easy to remove. The disadvantages are the presence of an external device that causes apprehension in the patient and a high rate of pin-track infections. The possibility of refracture, delayed union, or overgrowth are also some of the reported disadvantages1,2,5,6,12). Aronson and Tursky1) reported the results of EF in 44 pediatric femur fractures. They achieved bone union over an average of 10 weeks, a 10% rate of pin-track infections, and 5.8 mm of overgrowth. Kim et al12) reported that they required an average of 10 weeks for bone union and noted 4.8 mm of overgrowth and 2 cases of refracture. In this study, bone union took an average of 11.2 weeks, and 3.8 mm overgrowth was observed in the 3 cases (23%) with a pin track infection. One patient had pin breakage and 1 patient sustained a refracture after pin removal, which delayed the average time of bone union. It was assumed that the insufficient dynamization of the external fixator might have shielded the fracture site from the forces necessary to encourage sufficient callus formation, which led to refracture after removing the device.
FIN allows the early recovery of knee joint motion and weight bearing. In addition, it preserves the circulation around the fracture site, which promotes bone union because it works as an internal splint to maintain the length and alignment of the femur. However, migration of the nail, skin irritation, and bursitis over the insertion site are some of the complications reported2,3,7,8,10,11,13,15). Flynn et al8) reported that full weight bearing without a brace was possible within an average of 8.5 weeks in 58 pediatric femur fractures using FIN but irritation of the soft tissue by a prominent nail tip occurred in 4 cases, and refracture after premature of the nail occurred in one case. However, there was no significant leg-length discrepancy >2 cm or angular deformity >10. Yun et al.15) reported that full weight bearing without a brace was possible within an average of 8.4 weeks in 28 femoral fractures. Five cases showed an angular deformity >5 and 2 cases showed leg length discrepancy >1 cm. One fixation failure and one deep soft tissue infection at the entry point of the nail were some complications.
Similarly, in the 15 cases of pediatric femur fractures in this study, full weight bearing without a brace was possible within an average of 9.1 weeks. One case of nail migration occurred but there was no infection, fixation failure, angular deformity, or soft tissue irritation occurred. In the last follow up radiographs, 4.2 mm of overgrowth was shown but did not affect the gait, and no angular deformity >5 was observed. In previous studies, weight bearing was begun early. However, in this study partial weight bearing was started after callus formation on the radiograph and full weight bearing was started after bone union, which is believed to have prevented the angular deformity. In addition, the tip of the nail was close enough to the cortex so as not to irritate the surrounding soft tissues.
The acceptable degree of angular deformity or leg length discrepancy after bone union differs from surgeon to surgeon but for children aged between 5 to 10 years, less than 10 varus angulation and a 2 cm leg length discrepancy is considered generally acceptable, as reported by McCartney et al14). In our study, no patient in the FIN group showed angular deformity >5. The maximal overgrowth was 11 mm but this did not disturb the gait. For the EF group, the maximal overgrowth was 10 mm, and two patients showed an angular deformity between 5 to 10. However, no patient showed a gait disturbance.
Bar-On et al2) reported that in the FIN group, the parents' satisfaction with the treatment was much greater and full weight bearing was possible earlier than in the EF group. In addition, in the EF group, refracture, pin site infection, quadriceps atrophy and angular deformity were some of the complications encountered. In this study, there were no significant differences between the two groups in the last follow up but similar complications to those reported elsewhere occurred in the EF group during the process.
CONCLUSION
In this study femoral shaft fractures were treated with either EF or FIN with Ender nails in children aged between 6 and 11 years. The FIN and EF groups showed similar results at the last follow up. However, in the EF group, refracture, pin site infection, quadriceps atrophy and angular deformity were some of the possible complications during the healing process.
FIN is recommended for pediatric femoral shaft fractures, which require surgery, and EF should reserved for open or severely comminuted fractures.

 XML Download
XML Download