

 PDF
PDF ePub
ePub Citation
Citation Print
Print


Syphilitic bony lesions are unfamiliar to most physicians, and destructive lesions in the clavicle are more likely to be viewed initially as being indicative of malignant diseases. For this reason, patients may have to bear these diseases without a correct diagnosis for some time. However, adequate antibiotics like penicillin can easily control these diseases without sequelae. Despite the rarity of syphilis, it should be suspected because syphilitic osteomyelitis barely responds to other conventional treatments.
CASE REPORT
A 51 year-old woman with a painful swelling of the right clavicle that had not subsided for more than two months was transferred from a local clinic. She also complained of intermittent pain in the upper part of right anterior chest. A diffusely swollen mass was noticed during physical examination at the medial one third of the clavicle with erythematous overlying skin. When palpated, the mass was firm and tender and warmer than surrounding tissues, whilst her body temperature was normal.
The right shoulder showed a full range of passive motion but active motion was limited by pain at the clavicle.
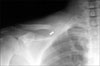
WBC, ESR and CRP counts were 9,940/mm3, 65 mm/hr and 2.8 mg/dl, respectively. Plain X-ray showed bony enlargement with destructive changes at the medial third of the right clavicle with severe soft tissue swelling (Fig. 1). MRI also revealed destructive bony changes and soft tissue swelling without definite fluid collection. The differential diagnoses offered by our radiologist were of malignant tumors, i.e., myeloma, lymphoma and metastatic tumor, and osteomyelitis.
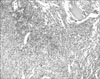
An incisional biopsy was performed to obtain an accurate diagnosis. A transverse incision was made over the medial third of the clavicle. Swollen soft tissue was dissected and the periosteum was opened. No abscess was found. However, the cortical bone had been severely destroyed and the marrow cavity was filled with granulation-like tissue. Some tissue from the marrow cavity and samples of destroyed bone were sent for pathological examination. Culture results were negative, but abundant lymphocytes and neutrophils were found, which suggested acute inflammation. However, no tumor cells were observed (Fig. 2). Because at this stage, we were unable to reach an accurate diagnosis, all available information was re-reviewed, and it was then found that her VDRL (qualitative study) was positive. Further serologic investigations, including TPHA (160x) and quantitative VDRL (1x) established a diagnosis of syphilis. FTA-ABS was reactive in IgG, while an IgM study revealed weak reactivity. Under a diagnosis of latent syphilis, benzathine penicillin G (2.4 million units) was administered once weekly for 3 weeks intramuscularly with oral concurrent doxycycline (200 mg weekly) for the 3 week period.
After the third injection of penicillin, her CRP level reduced to the normal range (0.22 mg/dl), and her ESR reduced to 25 mm/hr. Clavicular pain was also much improved. Follow-up X-ray showed some new bone formation at the site of cortical destruction. VDRL remained positive but was weaker than during the pretreatment state (2x). A later follow-up X-ray showed consolidation of newly formed bone. At the final 8-month follow-up, the patient complained no discomfort of the right clavicle or shoulder. Her CRP was 0.17 mg/dl and plain X-rays showed complete healing of the lesion without any evidence of infection (Fig. 3). The patient had denied throughout any history of venereal disease, but at the final follow-up, she told us that she had suffered from an ulcerative lesion on the external genitalia some years previously but had undergone no treatment.
DISCUSSION
The natural course of untreated syphilis follows three stages. The primary stage is characterized by chancre - ulcers on the genitalia, and in the secondary stage, various skin lesions, syphilids develop on the body, especially on face, shoulders, flank, palms and soles. The tertiary form is referred as neurosyphilis, so called tabes dorsalis. Moreover, the secondary and tertiary stages are separated by a latent asymptomatic period during which the only sign of underlying disease is a positive serology finding.
Congenital syphilis, which is transmitted in utero by a mother during early stage disease, is a well-known cause of various skeletal problems, such as, saber shin deformity in infancy3). The clavicle seems to be frequently involved in congenital syphilis, for example, 8 of 23 clavicular lesions identified in early childhood were attributed to congenital syphilis in a South African study7). Although destructive bone disease is a well-known problem of congenital and tertiary syphilis, osteitis and osteomyelitis may occur as complications of the earlier stages of acquired syphilis2).
Only a small proportion of patients with acquired syphilis progresses to late stage disease, and only 15% of those with late syphilis manifest gummatous lesions in skin or bone. Bony pathologies resemble those of periosteitis, osteitis, osteochondritis or osteomyelitis, and commonly involve tibia, cranial bones, shoulder girdle, femur, fibula, humerus and forearm6,8). However, spinal lesions are rare4). Syphilitic osteomyelitis usually develops in the metaphyseal area and may be visualized as periosteitis radiologically during the early stage1,9). Moreover, periosteal reactions result in new bone formation, and repetition results in sclerotic osteomylitis10).
Dismukes et al.2) described a 32-year-old man who suffered from malaise, fever, a chilling sensation, and right shoulder pain, and had positive serologic findings for syphilis. He was diagnosed as having secondary syphilis even though Treponema pallidum was not identified by culture of the specimen removed from his clavicular lesion. It was found that syphilitic osteomyelitis is marginally more common around the sternoclavicular joint and that it is highly sensitive to parenteral penicillins.
A diagnosis of syphilis requires a detailed analysis of medical history, progression of the illness which is not affected by the ordinary antibiotic therapy, radiologic findings, serologic studies and biopsy histologic findings. However, the diagnosis of syphilis is not straightforward because most patients are unwilling to reveal a history of venereal disease10), which is believed to be related to shame and partly to ignorance of the link between bone problems and venereal disease. Yusuf et al.10) reported syphilitic osteomyelitis in a 28-year-old febrile man with a large, firm, tender swelling in his mandible. He was a homosexual and had been treated for genital disease a few years previously, but failed to report this history. Our patient also denied a history of venereal disease during an early interview. However, at final follow-up, she told us of the ulcerative genital lesion that she had experienced some years before.
Serologic studies are of central importance for a diagnosis of syphilis, but a positive VDRL finding is often overlooked in laboratory reports, because false positive results are frequently encountered, such as, in the presence of connective tissue disease. Histologic examinations of lesion tissues show lymphocytes and plasma cells with various degrees of fibrosis8).
The osseous lesions of syphilis are highly sensitive to parenteral penicillins, and clinical symptoms, such as, pain and swelling, are rapidly resolved within 48 hours. However, radiological improvements are slow, although healing is usually complete and residua are rare2).
Syphilis is a disease that is easily treated but difficult to identify. To diagnose syphilitic osteomyelitis at an early stage, it is important that the possibility of syphilis is suspected and that specific serologic studies are conducted.

 XML Download
XML Download