

 PDF
PDF ePub
ePub Citation
Citation Print
Print


Chondroblastoma (CB) is a rare uncommon benign bone lesion accounting for <1% of all bone tumors7). It is defined as a benign, cartilageproducing neoplasm and a lytic bone lesion with a predilection for the epiphyseal region of the long bones in skeletally immature individuals7). Although almost 50% of the chondroblasoma cases involve the metaphysis, CB arising in the distal phalanx is extremely rare3). The authors report a case of CB arising from the distal phalanx of the great toe.
CASE REPORT
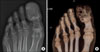
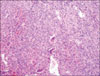
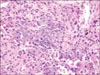
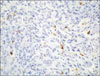
An 82-year-old woman presented with pain over her left great toe with a 1-year duration. She denied a history of prior trauma. An examination revealed pain upon pressure over the left great toe and a skin ulcer measuring 0.5 cm in diameter. The patient had no fever or other clinical symptoms. The radiographic findings showed an expansile osteolytic lesion with cortical thinning out and coarse trabeculation replacing the distal phalanx of the left great toe (Fig. 1), suggesting a benign bone tumor, such as a giant cell tumor, a giant cell proliferative granuloma, chondromyxoid fibroma, osteoblastoma, and aneurysmal bone cyst. An incisional biopsy and curettage were performed. The biopsy specimen contained uniform, round to polygonal cells with clear to slightly eosinophilic cytoplasm and round to ovoid nuclei (indicative of chondroblasts), intermingled with randomly distributed osteoclast-type giant cells (Fig. 2). The nuclei often showed longitudinal grooves and contained one small to inconspicuous nucleolus. In some areas, a fine network of pericellular calcification, which is known as "chicken wire calcification", was observed (Fig. 3). Mitoses were observed but the atypical forms were not observed. The specimen showed the typical features of a chondroblastoma. Some mononuclear cells were immunoreactive for the S-100 protein (Fig. 4).
After the biopsy, curettage and bone cement insertion were performed. There was no sign a recurrence or a mass observed by a radiological examination performed 2 years after surgery.
DISCUSSION
Codman2) first described chondroblastoma (CB) as an epiphyseal chondromatous giant cell tumor. Jaffe and Lichtenstein later renamed the condition as benign chondroblastoma4). CB is defined as a benign, cartilage-producing neoplasm that usually arises in the epiphyses of skeletally immature patients7), and accounts for <1% of all bone tumors.
CBs are reported to be eccentric, oval or round well-defined lesions mainly involving the epiphyseal region of the long bones, such as in the proximal portion of the femur, tibia or humerus. Equivalent sites within the flat bones such as the acetabulum of the pelvis, and ilium are relatively rare. Other unusual sites of involvement include the scapula, spine, ribs, patella, and occasionally the craniofacial bones6). Davila et al.3) reviewed CB of the hand and feet and reported CB arising in the phalanx in only 1 out of 25 cases. Moreover, CB arising from the distal phalanx of the toe is extremely rare5). Histologically, CB is a hypercellular tumor that consists of uniform, round to polygonal cells with well-defined cytoplasmic borders, slightly eosinophilic cytoplasm, and a round nucleus. These cells are packed in a pseudolobulated pattern in a chondroid matrix. In addition, a fine network of pericellular calcification, known as "chicken wire calcification", is also evident. Randomly distributed osteoclast-type giant cells are almost always present7). The contiguous involvement of the metaphyseal region occurs frequently6).
Several studies have concluded that CB is derived from epiphyseal cartilage cells8,10). A recent study on cartilage growth-plate-signaling molecules9) reported that CB is a neoplasm originating from mesenchymal cells committed toward chondrogenesis via the active growth plate signaling pathways. This can explain the close relationship between the growth plate cartilage and the epimetaphyseal location in CB. However, in the present case, CB arose in the great toe of an elderly woman. Brien et al. provided a reasonable explanation for this unusual location1). They suggested that CB is derived from multipotential mesenchymal cells of the tendon sheath, which have a tendency toward chondroid formation. The finding in this case supports this suggestion.
The authors reported a CB in the distal phalanx of the great toe. This case might provide a clue for the origin of CB.
 XML Download
XML Download