

 PDF
PDF ePub
ePub Citation
Citation Print
Print


INTRODUCTION
Displaced fractures of the tibial eminence of the tibia are an uncommon type of injury. However, this fracture can occur as a result motor vehicle accidents and sport injuries15). The injury mechanism is a twist, hyperflexion, hyperextension, varus or valgus force on the knee joint. The mechanism of the injury and appropriate treatment are unclear. With stress, the incompletely ossified tibial eminence in a child fails before ligament rupture. The integrity of the ACL is compromised. The fracture often extends into the weight-bearing portion of the articular surface of the medial tibial plateau. Pringle first reported avulsion of the anterior tibial spine in children in 19072). Meyer and McKeever presented a series of 45 patients including 35 children. These authors classified anterior eminence fractures into three types: type I, nondisplaced; type II, partially displaced or hinged; and type III, completely displaced12).
The treatment of types I and II fractures is relatively straightforward, and there is widespread consensus that external splintage is the ideal management4,5,7). However type III fractures often require an open reduction and internal fixation (ORIF). Meyer and McKeever recommended ORIF for all type II and III injuries, but more recently others have advocated a more conservative approach12,13).
Arthroscopic reduction and fixation using Kirschner wires or small fragment screws not crossing the epiphyseal plate has also provided good results.
The study investigated the clinical and radiological outcomes associated with arthroscopic cannulated screw fixation for all types II and III fractures and developed a treatment protocol based on these findings.
MATERIALS AND METHODS
Ten cases of displaced tibial eminence fractures who treated with arthroscopic internal fixation were reviewed both clinically and radiographically after an average follow-up of 22.4 months (range, 12 to 81 months). The fractures occurred due to road traffic accidents (5 patients ), falling down (2 patients)and sports injuries including skiing (2 patients) and skating (1 patient).
The fractures were classified using Meyer and McKeever's classification. All the patients with displaced fractures, types II and III, were operated on as soon as possible. There were two cases of associated intra-articular injuries, such as lateral and medial meniscal tears. However, none of the ten patients sustained collateral ligament or PCL injuries.
Through a high anterolateral and anteromedial approach for scope and hook insertion, a Kirschner wire was introduced through a medial parapatellar approach and drilled through the anterior edge of the displaced fragment (Fig. 1). Medial placement of the screw is preferred in cases of an avulsion of the anterior cruciate ligament, which includes a part of the medial tibial condyle. Care was taken to avoid the physis of the proximal tibia. Through a large-bore cannula, a cannulated drill (3.5 mm, 4.0 mm) was passed down over the Kirschner wire. The drill ends in a fork that can also be used to press the displaced fragment down. The epiphysis of the tibia was recessed by introducing the screw to the fracture site. The guidewire and screw were placed through the medial parapatellar approach under fluoroscopic control.
Although synovial leakage is a rather rare complication after a normal arthroscopic procedure, the leg is protected for 1 week postoperatively with an above-knee plaster cast to prevent synovial leakage. Post-operative rehabilitation of knee of range of motion of 0-30° and 0-90° was allowed 2 and 4 weeks after surgery, respectively. Weight bearing was allowed as tolerated, and a night locking brace in full extension was applied. The stability of the knee was evaluated manually. A Lachmann test was performed, and the range of motion and quadriceps weakness were checked. All the patients were interviewed according to the Lysholm functional score. All the screws were removed within 4-12 months after surgery. No complications were encountered after removing these screws.
RESULTS
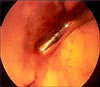
We treated a total of 10 patients from February 1997 to October 2005. There were 4 type II and 6 type III fractures. The mean age was 10.5 years (range, 7 to 13 years). And there were 4 males and 6 females. There were no associated injuries in type II lesions, and there were 2 cases of a lateral and medial meniscal rupture in the type III group. One patient with a type III lesion showed a shelf-like projection of bone in the area of the anterior spine on radiographs (Fig. 2). Under arthroscopy, an avulsion of the ACL (Fig. 3) was observed. This patient had some minor extension lag of approximately 10°,and the other patients showed a full range of motion without extension lag. One case was a radial tear on the medial meniscus (Fig. 4A) and an avulsed bony fragment (Fig. 4B) was found. An arthroscopic partial menisectomy was performed and the bony fragment was repositioned by pushing using an elevatorium. When the cannulated screw was removed, the ACL was appeared within the normal limit and the fixation of bony fragment kept firm and with no nonunion. The bed of the tibia from which the fragment had been avulsed was covered with mild fibrous tissue.
The clinical examination revealed all patients with type II and III lesions to have a negative Lachman test and no quadriceps weakness except one patient in the type III group (Table 1). The functional assessment using the Lysholm score was an average of 96.3 (min92.6-max99.0) for the type II (98.1) and type III (94.9), respectively. All patients had resumed their full activity by 12 months. No clinically detectable retropatellar chondromalacia was observed in this series.
DISCUSSION
Meyer and McKeever11,12) originally classified this fracture into three subgroups according to the severity. Zaricznyj16) added a fourth type with comminuted fragments. The general treatment of types I and II was conservative treatment using a long leg cast, type III and IV is a surgical reduction and internal fixation. However, the treatment for complete separation (type III) has been controversial since Pringle's (1907) first attempt at an open reduction16). Various modes of reduction and fixation have been proposed for these fractures. In the present study, if the fragment size is large enough and non-comminuted, the type II fracture fixed with a cannulated screw because it is possible to have persistent instability or a conversion to type III.
Under arthroscopy, Ando and Nishihara3) performing simple and firm bone fixation with minimal invasion using cannulated screws. They suggested that a fracture of the tibia be treated with interbone fixation under arthroscopy as long as the bone fragment remains mobile. In the present series, three displaced tibial eminence fracture of tibia (type IIIA) were treated by arthroscopy assisted cannulated screw fixation. This report described the technique of arthroscopic reduction and internal fixation used in these three cases.
Quite recently, various arthroscopic managements of a displaced tibial eminence fracture were reported6,9,10,14). These techniques each have an advantage or disadvantage. Arthroscopic reduction and percutaneous pinning is to perform a simple reduction or bony fragment but their fixation power is relatively loose, and the fixation technique is difficult if the fracture fragment is comminuted10). An arthroscopic pull-out suture is indicated for smaller comminuted fragments1,6). However, this technique is difficult to perform.
Arthroscopic internal fixation using a cannulated screw is to perform a simple and firm bone fixation. This method allows early motion. However, screw insertion is possible provided the fragment is >15 mm3). This method is not indicated for cases with small and comminuted fragments. In our three cases, cannulated screw fixation was indicated because the fragment size was long enough and non-comminuted. Ando and Nishihara3) recommended the direction of fixation from the metaphysis of the proximal tibia to the articular surface (retrograde). However, in the present study, its direction was from the articular surface to the proximal tibia (antegrade). This fixation technique was firmer than retrograde fixation, when the cannulated screw was located at 45° of knee flexion. The screw head did not crack the tibial notch of the femur. However, care must consider be taken to prevent any articular damage during the procedure. Two cannulated screws were used if the bone fragment was enough size to fixation. Under arthroscopy, a reduction of fragment was performed using arthroscopic probe or towel clip1). In this manner, satisfactory reduction was obtained with a <2 mm offset10).
When there was a fracture of the tibial eminence, Clanton et al8) reported an associated tear of the lateral. However, in this study, two of the ten cases showed a radial tear of the medial meniscus and a peripheral tear of the lateral meniscus. The frequency of an MCL injury is unclear10,14). In this study, there was no case of MCL injury. Nevertheless, a valgus stress test must be performed after aspirating the hemarthrosis10). A positive Lachman test in the presence of a fracture of the tibial eminence is indicative of an associated rupture of the MCL10).
The prognosis is relatively poor if the tibial eminence fracture has an associated ligamentous injury10,12). However, in this study, all cases showed excellent and good results. An acceptable range of immobilization was reported to be approximately 20-25° flexion10,16), and an approximately 20° flexion state immobilization is recommended. Ando and Nishihara recommended that partial weight bearing with a brace be started after 6 weeks and full weight bearing after 8 weeks2).
In this study, post-operative rehabilitation of knee range of motion of 0-30° and 0-90° was allowed 2 and 4 weeks after surgery, respectively. Weight bearing was allowed where tolerable, and a night locking brace in full extension was applied.




 XML Download
XML Download