

 PDF
PDF ePub
ePub Citation
Citation Print
Print


Abstract
Purpose
The purpose of this prospective study was to determine the factors that can be used to predict the postoperative range of motion, and to evaluate the short-term clinical results after total knee arthroplasty (Superflex™, Stryker Howmedica Osteonics, Allendale, NJ, USA).
Materials and Methods
A total of 69 patients (98 knees) were included in this study. The same surgeon performed all the procedures between April 2002 and December 2002. The patients age ranged from 53 to 81 years, with an average of 68.1 years. The preoperative and postoperative factors (BMI, preoperative flexion contracture, preoperative ROM, preoperative femoral-tibial angle, postoperative knee score and function score) influencing the ROM were evaluated. The patients were followed up once per 1 month for up to 3 years.
Results
At the last follow-up, the average flexion was 128° (110-145°). Twenty patients could kneel down comfortably. Fifty-two patients could sit cross-legged. The preoperative range of flexion was the most important factor influencing the ROM . The average Knee Society knee score was 96 points (80-100), and the function score was 93.6 points (60-100).
Figures and Tables
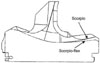 | Fig. 1Cross-section schematic diagram showing the difference between the Scorpio and Superflex tibial inserts. The major difference is the larger posterior radius for the Scorpio™ insert. Note that the Superflex™ has a lower posterior lip.
|

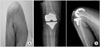 | Fig. 3A 67-year old female could flex 145° at the operated left knee (A) and anteroposterior and full flexion lateral X-ray (B).
|


Table 2
Comparison between the Postoperative ROM and the Factors at the 3-year Follow-up (Multiple Regression Analysis Test)

![]()


References
1. Anouchi YS, McShane M, Kelly F Jr, Elting J, Stiehl J. Range of motion in total knee replacement. Clin Orthop Relat Res. 1996. 331:87–92.

2. Cho SH, Ha YC, Song HR, et al. High Flex knee arthroplasty and range of motion. J Korean Orthop Assoc. 2004. 39:662–667.
3. Cho WS, Park JH, Kim JM, Hwang WY, Nam TS. Factors affecting range of motion after total knee arthroplasty. J Korean Orthop Assoc. 2003. 38:683–688.
4. Edwards E, Miller J, Chan KH. The effect of postoperative collateral ligament laxity in total knee arthroplasty. Clin Orthop Relat Res. 1988. 236:44–51.
5. Fehring TK, Valadie AL. Knee instability after total knee arthropasty. Clin Orthop Relat Res. 1994. 299:157–162.
6. Insall JN, Dorr LD, Scott RD, Scott WN. Rationale of the Knee Society clinical rating system. Clin Orthop Relat Res. 1989. 248:13–14.
7. Insall JN, Hood RW, Flawn LB, Sullivan DJ. The total condylar knee prosthesis in gonarthrosis. A five to nine-year follow-up of the first one hundred consecutive replacements. J Bone Joint Surg Am. 1983. 65:619–628.
8. Kanekasu K, Banks SA, Honjo S, Nakata O, Kato H. Fluoroscopic analysis of knee arthroplasty kinematics during deep flexion kneeling. J Arthroplasty. 2004. 19:998–1003.
9. Lizaur A, Marco L, Cebrian R. Preoperative factors influencing the range of movement after total knee arthroplasty for severe osteoarthritis. J Bone Joint Surg Br. 1997. 79:626–629.
10. McAuley JP, Harrer MF, Ammeen D, Engh GA. Outcome of knee arthroplasty in patients with poor preoperative range of motion. Clin Orthop Relat Res. 2002. 404:203–207.
11. Myles CM, Rowe PJ, Walker CR, Nutton RW. Knee joint functional range of movement prior to and following total knee arthroplasty measured using flexible electrogoniometry. Gait Posture. 2002. 16:46–54.
12. Ritter MA, Montgomery TJ, Zhou H, Keating ME, Faris PM, Meding JB. The clinical significance of proximal tibial resection level in total knee arthroplasty. Clin Orthop Relat Res. 1999. 360:174–181.
13. Rorabeck CH, Bourne RB, Lewis PL, Nott L. The Miller-Galante knee prosthesis of the treatment of osteoarthritis. A comparison of the results of partial fixation with cement and fixation without any cement. J Bone Joint Surg Am. 1993. 75:402–408.
14. Schurman DJ, Parker JN, Ornstein D. Total condylar knee replacement. A study of factors influencing range of motion as late as two years after arthroplasty. J Bone Joint Surg Am. 1985. 67:1006–1014.
15. Stern SH, Insall JN. Total knee arthroplasty in obese patients. J Bone Joint Surg Am. 1990. 72:1400–1404.
16. Tew M, Forster IW, Wallace WA. Effect of total knee arthrolasty on maximal flexion. Clin Orthop Relat Res. 1989. 247:168–174.
17. Warren PJ, Olanlokun TK, Cobb AG, Walker PS, Iverson BF. Laxity and function in knee replacements. A comparative study of three prosthetic designs. Clin Orthop Relat Res. 1994. 305:200–208.
18. Yamakado K, Kitaoka K, Yamada H, Hashiba K, Nakamura R, Tomita K. Influence of stability on range of motion after cruciate-retaining TKA. Arch Orthop Trauma Surg. 2003. 123:1–4.
19. Yamazaki J, Ishigami S, Nagashima M, Yoshino S. Hy-Flex II total knee system and range of motion. Arch Orthop Trauma Surg. 2002. 122:156–160.
 XML Download
XML Download