

 PDF
PDF ePub
ePub Citation
Citation Print
Print


INTRODUCTION
Müller first described the congenital absence of the unilateral lumbosacral articular process8). Although rare, this absence has been incidentally noted in patients with back pain. Accordingly, these patients are not indicated for corresponding surgery. In some cases, segmental instability causes occasional lower back pain.
In the atlas, congenital defects of the posterior arch are uncommon, and clefts of the posterior arch are found with an incidence of 4%4). Being asymptomatic in most cases, congenital defects of the posterior arch are found incidentally. In some cases, however, a variety of neurological symptoms has been reported2).
To the best of our knowledge, we have encountered a unique case of a coincidental congenital complete absence of the posterior arch of the atlas and the unilateral lumbosacral articular process. We report this case with a review of the literature.
CASE REPORT
A 21-year old male patient presenting with severe back and left buttock pain was brought to the emergency room. The patient had immediate pain in the lower lumbar area but denied having any neurological symptoms. He had experienced these symptoms intermittently for three years. A physical examination revealed tenderness in the lower lumbar spine. There was neither motor weakness nor a sensory defect. No pathological reflexes were noted. Lasègue's test was negative. The patient underwent plain radiography of the lumbar spine in an erect position. Subsequently, anteroposterior, lateral and dynamic views were obtained in the neutral position and during extension and flexion of the lumbar spine. On plain radiography, congenital absence of the unilateral lumbosacral articular process was seen on the left side. In addition, there was no segmental instability (Fig. 1). Computerized tomography confirmed the congenital absence of the left lumbosacral articular process (Fig. 2). Contrast-enhanced magnetic resonance revealed disc degeneration at L5-S1, with no evidence of disc herniation. Magnetic resonance imaging also confirmed congenital absence of the left unilateral lumbosacral articular process (Fig. 3). The back and left buttock pain subsided with an epidural nerve block at L5-S1. The patient then returned to work as a swimming coach while taking analgesics and muscle relaxants as an intermittent medication.
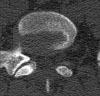
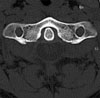
Six months later, the patient was admitted to the emergency room with severe neck pain and suboccipital headaches. There was no history of specific trauma. During hospitalization, the patient presented with a persistent stiff neck and suboccipital headaches. He occasionally had a reproducible Lhermitte sign with neck extension. There was neither motor weakness nor a sensory deficit on the upper and no dysfunction of the lower extremities, bowel or bladder. To visualize the cervical spine, the patient initially underwent plain radiography, computerized tomography and contrast-enhanced magnetic resonance imaging. Plain radiography and computerized tomography revealed the congenital complete absence of the posterior arch of the atlas (Fig. 4, 5). There was no instability at C1-C2 (Fig. 6). Magnetic resonance imaging revealed the congenital complete absence of the posterior arch of the atlas (Fig. 7). Furthermore, magnetic resonance imaging revealed neither compression nor an abnormal density in the same level of the spinal cord (Fig. 7). On brain magnetic resonance imaging, there was no specific lesion.
The patient was noted to have the congenital absence of the posterior arch of the atlas, as well as the unilateral lumbosacral articular process. To identify the presence of other congenital anomalies, the patient underwent not only abdominal and cardiac ultrasonography but also abdominal computerized tomography. However, these examinations revealed no other anomalies. On EMG, there was no specific neurological deficit. During hospitalization, the neck pain subsided. Upon discharge, the patient was prescribed a non-steroidal, anti-inflammatory drug.
DISCUSSION
In early fetal life, the sclerotome originating from the mesenchyme is destined to differentiate into the vertebra. Each vertebra has three primary ossification centers: one in the body and the other two in both sides of the neural arch. Secondary ossification centers for the apophyges are located at the ends of the spinous and transverse processes1). During ossification, an accessory center is sometimes involved in the ossification of the lamina of the inferior articular process9). Based on the literature, the congenital anomaly of the posterior spinal element may be interpreted as a failure of fusion between the primary ossification centers lying at the base of the articular facet.
The congenital absence of the unilateral lumbosacral articular process is caused by (a) a failure of ossification and (b) impaired ossification following an insufficient blood supply9). Without a separated neural arch, the absence of an articular process cannot be explained based on the concept of ossification failure.
In the lumbar spine, the anomalous location of the simple unilateral upper or lower articular process could not be specified. Of the defects noted between L5 and S1, the most common type was a unilateral defect of the upper facet associated with ipsilateral defect of the lower facet of the superjacent vertebra, i.e., a defect of the apophyseal joint5).
The congenital absence of the unilateral lumbosacral articular process changes the pathway of the biomechanical force transmitted through the spine during weight bearing. This change will eventually cause hypertrophy of the contralateral lamina and facet joint6). Hypertrophy of unilateral arch will be one of the major causes of lower back pain. As a cause of low back pain, the instability seems to not only change the structure but also minimize the rotational stress affecting intact apophyseal joints6). In this case, on computerized tomography and magnetic resonance imaging, hypertrophy of the unilateral arch was not seen on the contralateral side. Moreover, no segmental instability was noted in the lumbar spine.
In the atlas, there are three ossification centers: one for the anterior tubercle and two for the lateral masses and the posterior arch4,10). Two centers located in the lateral masses are responsible for the ossification of the posterior arch of the atlas4,10). The defect of the posterior arch is explained by a failure of local chondrogenesis rather than subsequent ossification7). In the atlas, anomalies of the posterior arch, which are regarded as a developmental insufficiency, range from partial absence (i.e., median, unilateral and bilateral clefts) to complete absence3,10). In the atlas, the partial absence in which the posterior arch is slightly discontinued at midline is common. However, the complete absence of the posterior arch is rarely noted. Whether partial or complete, the absence of the posterior arch has been reported to be associated with the developmental disorder in cartilaginous reformations and not a disturbance in the ossification per se.
Although rare, a defect of the posterior arch is incidentally noted as an asymptomatic variant on routine radiography of the cervical spine. Generally, the congenital absence of the posterior arch is regarded as an asymptomatic finding. However, the structural instability may be the cause of the atlantoaxial instability and neurological deficits2,10). In this case, the complete absence of the posterior arch was noted without atlantoaxial subluxation and instability on plain radiography. Computerized tomography is a useful tool for assessing the extent and status of this anomaly. Magnetic resonance imaging enables one to evaluate the integrity of neural structures.
We recommend that evaluations of the other spinal regions are needed, in case of an anomaly of the posterior element of the cervical or lumbar spine.





 XML Download
XML Download