

 PDF
PDF ePub
ePub Citation
Citation Print
Print


Abstract
Purpose
The purpose of this study was to compare the clinical results of a high-flex design (Scorpioflex®, Stryker) in total knee arthroplasty with those of a non-high-flex design (Scorpio® PS type, Stryker).
Materials and Methods
Fifty-two knees with at least 120 degrees of further flexion preoperatively underwent total knee arthroplasty. Of the 52 knees, there were 35 knees in the high-flex design (HF group) and 17 knees in the non high-flex design (non-HF group). The clinical results were evaluated by postoperative further flexion at 3 months, 6 months, 1 year, 2 years and 3 years, as well as by Delta flexion, which means postoperative flexion improvement. The Knee Society Score and X-rays were evaluated preoperatively and at the 3-year follow-up.
Results
The HF group showed significantly greater flexion than the non-HF group at 3 months postoperatively (p=0.000). The delta flexion was also greater in the HF group at 3 months postoperatively (p=0.000). The Knee Society Score and X-rays were similar in the two groups at the final follow-up (p>0.05).
Figures and Tables
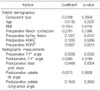
Table 1
A Comparison of the Preoperative Variables between the High-flex and Non High-flex Total Knee Arthroplasty Groups
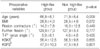
Table 2
Comparison of the Further Flexion between the High-flex and Non High-flex Total Knee Arthroplasty Groups

Table 3
Comparison of the Delta Flexion between the High-flex and Non High-flex Total Knee Arthroplasty Groups


References
1. Anouchi YS, McShane M, Kelly F Jr, Elting J, Stiehl J. Range of motion in total knee replacement. Clin Orthop Relat Res. 1996. 331:87–92.

2. Cho SH, Ha YC, Song HR, et al. High flex knee arthroplasty and range of motion. J Korean Orthop Assoc. 2004. 39:662–667.
3. Cho WS, Park JH, Kim JM, Hwang WY, Nam TS. Factors affecting range of motion after total knee arthroplasty. J Korean Orthop Assoc. 2003. 38:683–688.
4. Davies DM, Johnston DW, Beaupre LA, Lier DA. Effect of adjunctive range-of-motion therapy after primary total knee arthroplasty on the use of health services after hospital discharge. Can J Surg. 2003. 46:30–36.
5. Dennis DA, Komistek RD, Stiehl JB, Walker SA, Dennis KN. Range of motion after total knee arthroplasty: the effect of implant design and weight-bearing conditions. J Arthroplasty. 1998. 13:748–752.
6. Gatha NM, Clarke HD, Fuchs R, Scuderi GR, Insall JN. Factors affecting postoperative range of motion after total knee arthroplasty. J Knee Surg. 2004. 17:196–202.
7. Huang HT, Su JY, Wang GJ. The early results of high-flex total knee arthroplasty: a minimum of 2 years of follow-up. J Arthroplasty. 2005. 20:674–679.
8. Insall JN, Dorr LD, Scott RD, Scott WN. Rationale of the knee society clinical rating system. Clin Orthop Relat Res. 1989. 248:13–14.
9. Insall JN, Hood RW, Flawn LB, Sullivan DJ. The total condylar knee prosthesis in gonarthrosis. A five to nine-year follow-up of the first one hundred consecutive replacements. J Bone Joint Surg Am. 1983. 65:619–628.
10. Kim YH, Sohn KS, Kim JS. Range of motion of standard and high-flexion posterior stabilized total knee prostheses. A prospective, randomized study. J Bone Joint Surg Am. 2005. 87:1470–1475.
11. Lizaur A, Marco L, Cebrian R. Preoperative factors influencing the range of movement after total knee arthroplasty for severe osteoarthritis. J Bone Joint Surg Br. 1997. 79:626–629.
12. McAuley JP, Harrer MF, Ammeen D, Engh GA. Outcome of knee arthroplasty in patients with poor preoperative range of motion. Clin Orthop Relat Res. 2002. 404:203–207.
13. Myles CM, Rowe PJ, Walker CR, Nutton RW. Knee joint functional range of movement prior to and following total knee arthroplasty measured using flexible electrogoniometry. Gait Posture. 2002. 16:46–54.
14. Ritter MA, Harty LD, Davis KE, Meding JB, Berend ME. Predicting range of motion after total knee arthroplasty. Clustering, log-linear regression, and regression tree analysis. J Bone Joint Surg Am. 2003. 85:1278–1285.
15. Schurman DJ, Parker JN, Ornstein D. Total condylar knee replacement. A study of factors influencing range of motion as late as two years after arthroplasty. J Bone Joint Surg Am. 1985. 67:1006–1014.
16. Tew M, Forster IW, Wallace WA. Effect of total knee arthroplasty on maximal flexion. Clin Orthop Relat Res. 1989. 247:168–174.
17. Yamazaki J, Ishigami S, Nagashima M, Yoshino S. Hy-Flex II total knee system and range of motion. Arch Orthop Trauma Surg. 2002. 122:156–160.
 XML Download
XML Download