

 PDF
PDF ePub
ePub Citation
Citation Print
Print


INTRODUCTION
Several important tissues have unique magnetic susceptibility differences relative to surrounding tissues. Signals from these substances will become out of phase with background tissues at sufficiently long echo times. Thus phase imaging offers a means of enhancing contrast in magnetic resonance (MR) imaging. In 1997, it was possible to remove most of the unwanted phase artifacts and keep the local phase of interest (1). Combining the phase and the magnitude information made a new susceptibility weighted magnitude image, which is called today as susceptibility-weighted imaging (SWI) (2).
SWI is based on high-resolution, 3D, fully velocity-compensated gradient-echo sequences using both magnitude and phase images. To enhance the visibility of the venous structures, the magnitude images were multiplied with a phase mask generated from the filtered phase data, which are displayed at best after post-processing of the 3D dataset with the minimal intensity projection (minIP) algorithm.
This pictorial review is aimed at illustrating and discussing its main clinical applications.
MATERIALS AND METHODS
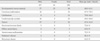
After obtaining local ethics committee approval, between March 2011 and February 2013, data in 200 consecutive patients who met the inclusion criteria for this study were retrospectively reviewed from our data base. Inclusion criteria were the following: 1) Patients underwent MR examinations that included SWI on a 3 tesla (T) MR imager, and 2) they had lesions of clinical significance and cerebrovascular pathology. Among the 200 patients, 80 showed developmental venous anomaly (DVA), 22 showed cavernous malformation, 12 showed calcifications in various conditions, 21 showed cerebrovascular accident (CVA) with susceptibility vessel sign or microbleeds, 52 showed brain tumors, 2 showed diffuse axonal injury (DAI), 3 showed arteriovenous malformation (AVM), 5 showed dural arteriovenous fistula (AVF), 1 showed moyamoya disease, and 2 showed Parkinson's disease (Table 1).
MR imaging was performed on a 3T (Siemens, Skyra, Erlangen, Germany) equipped with a 20-channel head coil. The imaging parameters for the SWI were: TR/TE = 28/20 ms, FA = 15°, BW = 120 Hz/pixel, spatial resolution = 0.3 × 0.3 × 1.2 mm3 and field-of-view = 230 mm.
RESULTS
Normal appearance of intracranial structures on SWI
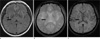
Figure 1 illustrates the normal appearance of intracranial structures on minIP SWI. The white matter slightly hyperintense to gray matter. The red nucleus, substantia nigra, lentiform nucleus and globus pallidi are low signal intensity due to iron deposition (Fig. 1). This becomes more pronounced with increasing age (Fig. 2) (3).
The small cortical veins are seen as linear low signal intensities due to signal loss from deoxyhemoglobin in venous blood. But, the major venous sinuses are of larger caliber with faster venous flow, and because they entirely occupy several voxels, there is no signal loss as with small subvoxel veins (4).
Developmental venous anomaly
DVA is considered to be incidental malformations of venous drainage patterns. There is no arterial component in this entity. Normal brain tissue is present between the veins comprising the lesion. DVA may represent the most common cerebrovascular malformation, accounting for 63% of vascular malformations in one large study, with an overall incidence of 2% (5). SWI can readily demonstrate the slow venous flow in these lesions and their characteristic curvilinear vascular channels receiving drainage from a spoke wheel-appearing collection of small, tapering veins arranged in a radial pattern (Fig. 3).
Cavernous malformation
Cavernous malformation represents a pathologic subtype of vascular malformation, appearing as discrete, compact, honeycomb like masses of endothelial-lined sinusoidal vascular spaces that contain essentially thrombosed blood. This lesions is congenital. The key features of T2-weighted image are focal central heterogeneity containing areas corresponding to subacute-chronic hemorrhage, circumferential complete rings of markedly hypointense iron-storage forms around these high-intensity central areas, no mass effect or edema (Fig. 4a, c). SWI has exquisite sensitivity for hemosiderin and calcification in theses lesions (Fig. 4b, d). Without SWI, small vascular malformations could be missed by conventional imaging techniques such as T2-weighted image, gradient recalled echo (GRE) (Fig. 4e, f, g).
Arteriovenous malformation
The most common clinically symptomatic cerebrovascular malformation is the AVM. AVM represents congenital anomaly of blood vessel development and result from preservation of direct communication between arterial and venous channels without an intervening capillary network (6). The nidus, that is the site of primitive communication which replaces the normal arterioles and capillaries, permits increased flow through the arterial feeding vessels to the AVM and delivers increased blood volume under relatively high pressure into the cerebral venous system. T2-weighted image demonstrates marked hypointensity along the surface of the brain parenchyma or along the ependymal surface of the ventricle in this entity (Fig. 5a). SWI can demonstrate the tangle of arterial feeding vessels and the enlarged draining veins as well as hemorrhage (Fig. 5b).
Calcification
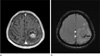
Computed tomography (CT) has long been considered the gold standard in detecting calcification. In conventional MRI such as spin echo T1- or T2-weighted images and GRE, calcifications usually appear as hypointense and cannot be differentiated from hemorrhage. MRI has been thought to be the best imaging modality in the central nervous system, but there are occasions when a CT scan needs to be obtained to confirm the presence of calcification suspected on MRI when it becomes a critical sign in diagnosis. It has been recognized that using phase helps to discriminate between calcium and iron because calcifications tend to be diamagnetic and iron paramagnetic, thus they appear with the opposite signal intensity in filtered phase images (Fig. 6) (7).
Cerebrovascular accident
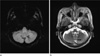
In case of acute ischemic stroke, the presence of prominent veins, microbleeds and the "susceptibility vessel sign" in SWI has been considered to be useful in evaluating stroke severity, treatment and prognosis (8). In acute stroke, presence of unpaired electrons in deoxyhemoglobin, methemoglobin within the occluded vessel gives them paramagnetic properties, which causes signal loss on MRI, which is best detected using T2*-weighted sequences - the so called "susceptibility vessel sign". The presence of prominent veins was hypothesized to be caused by the increased oxygen extraction fraction (OEF), which reflects the ratio of deoxyhemoglobin to oxyhemoglobin in the capillaries and veins. Since the OEF is increased in the penumbra following acute ischemic stroke, these hypointense signals shown by SWI could possibly represent the penumbra (Fig. 7). Acute infarction with subsequent tissue breakdown and reperfusion phenomenon can lead to secondary petechial hemorrhage. Demonstration of hemorrhage can alter clinical management. SWI has exquisite sensitivity for small foci of hemorrhagic transformation and microbleeds within the infarct.
Brain tumors
The development of SWI allows improved contrast and detection of both the venous vasulature and hemorrhage within tumors which cannot be seen with conventional imaging methods (Fig. 8) (4) and tiny hemorrhagic metastasis (Fig. 9).
The internal architecture of tumors varies significantly between SWI and contrast-enhanced T1-weighted image. Figure 10 shows an example of the internal vascular structure of a lesion that is not visible even with the use of a contrast agent on conventional MRI (Fig. 10). Internal architecture on contrast enhanced T1-weighted image is determined by the presence of necrosis, cysts, and tumor boundaries, whereas the internal architecture on SWI is determined mostly by blood products, either from spontaneous bleeding or from surgical trauma. This difference in image appearance can allow recurrent tumor to be distinguished from postsurgical changes (9).
Moyamoya disease
Moyamoya disease is an uncommon cerebrovascular disease characterized by progressive stenosis of the terminal portion of the bilateral internal carotid arteries and circle of Willis with bilateral involvement of the anterior cerebral arteries, MCAs and the posterior cerebral arteries that leads to the compensatory formation of an abnormal network of perforating blood vessels, named Moyamoya vessels, that provide collateral circulation. The clinical presentations are intracranial bleeding, transient ischemic attack or cerebral infarction.
Variable perfusion scan modalities such as single-photon emission computed tomography (SPECT), positron emission tomography (PET), Xenon-CT, and dynamic perfusion CT have been applied to predict the patients with severe hemodynamic impairments. Dynamic susceptibility contrast (DSC) MR perfusion imaging and ASL are available for quantitative hemodynamic analysis.
Neurodegenerative disease
Abnormal iron accumulation occurs in the brains of patients with various neurodegenerative diseases such as Parkinson's disease, multiple system atrophy, Alzheimer disease, and multiple sclerosis. MR imaging such as T2*-weighted image, GRE has been demonstrated to be an important tool to quantify iron content in vivo (13). SWI is a new technique that exploits the magnetic properties of iron content of tissues by using magnitude and phase images and would be a very sensitive imaging sequences, better elaborating putative iron distrubution or extent in the deep gray nuclei of patients with Parkinson's disease (Fig. 13).
Traumatic brain injury
SWI is helpful for the evaluation of traumatic brain injury, often associated with punctate hemorrhages in the deep subcortical white matter, which are not routinely visible on CT or conventional MR imaging sequences (Fig. 14). Study by Tong et al. (14) has shown that SWI has 3-6 times the sensitivity of conventional T2*GRE sequences for detecting the size, number, volume, and distribution of hemorrhagic lesions in DAI.
DISCUSSION
SWI is very useful in detecting neurovascular malformations such as DVA and cavernous malformation, in characterising brain tumors, in detecting cerebral microbleeds and in recognizing calcifications in various pathological conditions. The phase images are especially useful in differentiating between paramagnetic susceptibility effects of blood and diamagnetic effects of calcium. SWI can also be used to evaluate changes in iron content in neurodegenerative disorders and to predict stroke evolution.











 XML Download
XML Download