

 PDF
PDF ePub
ePub Citation
Citation Print
Print


INTRODUCTION
Most soft tissue tumors show high signal on T2-weighted images (T2WIs). Some tumors with the same histologic diagnoses showed different MR appearances in that some had a long T2 while others had a short T2 (1). Abundant collagen and marked hypocellularity or acellularity in a soft-tissue tumor or hemosiderin-laden masses result in a decreased signal on T2WI (1, 2). Lesions with decreased signal intensity (SI) on both T1- and T2WIs might represent densely mineralized lesions. And also thrombus, phlebolith, hemorrhage and fast blood flow can show low signal intensity on T2WI. We defined low SI on T2WI as signal intensity lower than that of fat or fluid and signal intensity equal, slightly higher or lower to that of skeletal muscle. The aims of this article are to differentiate soft tissue masses showing low SI according to the histopathologic findings, knowing components contributing to low signal intensity on T2WIs.
Components that could result in low signal intensity on T2WI
HIGH COLLAGEN COMPONENTS AND HYPOCELLULARITY
Fibrous lesion with high collagen contents
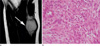
Fibroma of tendon sheath
Fibroma of the tendon sheath is a benign fibroblastic proliferation that occurs in the distal extremities often attached to tendon or tendon sheath (3). The MR imaging findings vary when areas with increased cellularity or myxoid change occur within the lesion (4). Low SI on T2WI can be attributed to the overall hypocelluarity and highly collagenous stroma found in this region (1, 3) (Fig. 1).
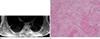
Nodular fasciitis
Nodular fasciitis is a benign soft tissue lesion characterized by proliferation of fibroblasts (5). Lesions having a myxoid matrix and hypercellularity in the early stage demonstrate higher SI than that of muscle on T1WIs and than that of fat on T2WIs. Mature lesions are often characterized by increased fibrosis, and the fibrotic areas present as markedly hypointense to the surrounding muscles on all pulse sequences (5, 6) (Fig. 2).
Desmoplastic fibroblastoma
Desmoplastic fibroblastoma is a fibrous soft tissue tumor. The low SI on T2WI is attributed to the low cellularity of the mass in a background of abundant collagen (7).
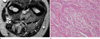
Fibromatoses
The fibromatoses are a diverse group of a soft tissue lesions that occur at different ages and anatomic locations and that have common histopathologic features (8). Fibromatosis in the proliferative phase demonstrates a high degree of cellularity and have a predominantly hyperintense signal on T2WIs. These lesions typically mature over time with increased collagen content and reduced cellularity, with a resultant decrease in SI on T2WIs (9) (Fig. 3).
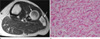
Malignant fibrous histiocytoma (MFH)
MFH is a pleomorphic sarcoma, although MFH now appears more related to the fibroblasts, myofibroblasts, or undifferentiated mesenchymal cells. Generally MFH demonstrates an intermediate SI on T1WIs and heterogeneous high SI on T2WIs reflecting the variable pattern seen histologically (10). These variations include regions with prominent fibrous tissue (high collagen content; low SI); calcification (low signal foci); hemorrhage (high signal on all pulse sequences; fluid levels), necrosis (low signal on T1WI and high signal on T2WIs); and areas of tumor with lower collagen content (intermediate on T1WI; high signal on T2WI) (11) (Fig. 4).
Elastofibroma
Elastofibroma is a degenerative or reactive fibrous pseudotumor that arises most commonly between the inferior margin of the scapula and posterior chest wall in elderly individuals (9). On both T1- and T2WIs, the lesion is well defined and has intermediate signal intensity similar to that of skeletal muscle, corresponding to areas of dense fibrous connective tissue with interlaced areas of SI similar to that of fat (12) (Fig. 5).
Fibrolipoma
Lipomas occasionally contain other mesenchymal elements. The most common of these is fibrous connective tissue, which may demonstrate a septal configuration, appearing as linear areas of decreased signal on MRI, regardless of pulse sequence (Fig. 6). When significant fibrous tissue is present, these lesions may be termed fibrolipoma.
Neurogenic lesion with high collagen contents
Traumatic neuroma
Traumatic neuromas develop from a nonneoplastic proliferation of the proximal end of a severed, partially transected, or injured nerve as a result of trauma or surgery. They typically have intermediate to high SI on T2WI. Their SI is often heterogeneous, with a ringlike pattern ("fascicular sign"), which correlates with the histologic morphology of nerve fascicles (13) (Fig. 7).
Schwannoma
Schwannomas are benign slow-growing encapsulated tumors of nerve sheath origin (13). Histologically they are composed of two cell types: Antoni A and Antoni B. The Antoni A cells are densely packed and arranged in fascicles, Antoni B cells are less compact and are prone to cystic degeneration. T2WIs corresponds histologically to peripheral myxomatous tissue and central fibrocollagenous tissue. Another intrinsic MR imaging characteristic, fascicular sign manifests as multiple small ringlike structures (with peripheral higher signal intensity) on either T2- or proton density-weighted MR images. This sign corresponds to the fascicular bundles seen pathologically in neurogenic neoplasms (13).
Neurofibroma
Neurofibromas are nonencapsulated, often infiltrative lesions (14). Diffuse type is a poorly defined lesion that spreads along connective tissue septa and surrounds rather than destroys adjacent normal structures. Skin and subcutaneous tissue involvement was most typical (15). They often show predominant low SI on T2WIs, may be related to the high collagen content of these lesions (13). When the central area of the tumor is composed of dense collagenous tissue, it has decreased SI on T2WIs, resulting in a characteristic "target" appearance (14) (Fig. 8).
HEMOSIDERIN
Giant cell tumors of the tendon sheath (GCTTS)
GCTTS is a benign proliferative lesion of synovial origin arising from the tendon sheath, joint capsule, bursa or ligaments (14). The MR imaging features are variably heterogeneous and depend on the relative proportions of fat, fibrous tissue, and hemosiderin, although the SI of lesions is predominantly low (14, 16). Typical lesions have areas of low SI on both T1- and T2WIs due to the paramagnetic effect of hemosiderin (14, 16).
MINERALIZATION
Synovial chondromatosis or osteochondromatosis
Synovial osteochondromatosis is a benign monarticular disorder of uncertain cause characterized by proliferation and metaplastic transformation of the synovium with formation of multiple cartilaginous nodules (17). MR imaging is characterized as lobulated, homogeneous, intermediate, intraarticular SI similar to that of muscle on T1WIs, with high signal intensity on T2WIs and focal areas of low SI with all pulse sequences. The areas of signal void corresponded to regions of calcification (18) (Fig. 10).
Myositis ossificans
Myositis ossificans (MO) is a benign, solitary, self-limiting, ossifying soft-tissue mass typically occurring within skeletal muscle. The MR imaging appearance changes with the age of the lesion, reflecting the evolving histologic characteristics. In the intermediate or older lesions, MR images showed curvilinear and irregular regions of decreased SI peripherally as well as within lesions, corresponding to mineralization seen on CT scans and radiographs. Areas of hemosiderin deposition from previous hemorrhage and fibrosis also may contribute to areas of decreased SI on both pulse sequences (19, 20) (Fig. 11).
THROMBUS, PHLEBOLITH, HEMORRHAGE AND FAST BLOOD FLOW
Intravascular papillary endothelial hyperplasia
Intravascular papillary endothelial hyperplasia (IVPEH) is a reactive proliferative lesion of endothelial cells within the vessels and is usually associated with thrombi. Hyperintense region on T2WI corresponded to the ectatic blood-pool space in the hemangioma as well as to isointense central regions composed of thrombosis and endothelial papillary proliferative tissue (22). T2 sequences may show low SI areas reflecting thrombotic or hemorrhagic material and low signal internal septae have been described (23) (Fig. 13).
Soft tissue hemangioma
Hemangioma is one of the most common soft tissue tumors and usually located superficially but may involve deep structures such as skeletal muscle. On T2WI, it shows areas that are very high SI due to vascular tissue and other regions that are intermediate in SI due to fat (24). Punctate or reticular low SI areas may be present, representing fibrous tissue, fast flow within vessels, or foci of calcification. Areas of thrombosis appear as circular low SI areas at MR imaging, similar to phleboliths (25).
Synovial sarcoma
Synovial sarcoma is a mesenchymal neoplasm of uncertain pathogenesis. MR images may demonstrate complex signal characteristics, with fluid levels, hemorrhage, and septation in the lesions. Pathologically triple signal appearance on T2WIs reflects the mixture of solid, cystic, fibrous, and hemorrhagic elements present in many synovial sarcomas (26).
Alveolar soft part sarcoma
Alveolar soft part sarcoma is a highly vascular malignant tumor which occurs most often in the soft tissues of the pelvis and lower limbs. On dynamic MRI, the margin of the tumor enhanced strongly in the early phase and washout occurred in the late phase. The signal void representing fast flow was shown at the margin of the tumor (27) (Fig. 14).
OTHERS
Lymphoma
Lymphomas are characterized pathologically by the proliferation of cells native to the lymphoid tissue-lymphocytes, histiocytes, and their precursors (29). At MRI extranodal soft-tissue lymphomas are homogeneously isointense or slightly hypointense relative to normal muscle on T1WIs and hyperintense to muscle on T2WIs (30). Lymphomas usually have homogeneously low SI on T2WIs because of their dense cellularity (31).
In conclusions, We described the possible disease entities that can show low signal intensity on T2-weighted image according to the composition of the soft tissue tumors. In addition to this, characteristic locations, morphology and signal intensities on other sequences may be helpful for the differential diagnosis of mostly nonspecific soft tissue masses on MRI.











 XML Download
XML Download