

 PDF
PDF ePub
ePub Citation
Citation Print
Print


INTRODUCTION
Multiple level spinal injuries have been recognized for some time (1,2,3,4,5,6,7,8,9,10). Previous studies using basic radiography have been used to evaluate these injuries, reporting frequencies of 4.2% to 23.8% (1,2,3,4,5,6,7,8,9,10), while more recent studies (11, 12) using magnetic resonance imaging (MRI) have reported a higher frequency. Calenoff et al. (4) designated these multiple spinal injuries as primary or secondary. A primary lesion is the vertebral injury first identified and initially considered to account for the patient's neurologic deficit (4). A secondary lesion is a vertebral injury unrecognized initially or which, when diagnosed simultaneously, was felt to have less neurologic significance than the primary lesion (4). Subchondral bone contusion (bone bruise, trabecular microfracture) has been accepted as the most common type of secondary lesion. In the spine, subchondral bone contusions are observed on MRI scans as band-like or diffuse zones of high signal intensity on T2 weighted sequences, and decreased signal intensity on T1 weighted sequences (13, 14). The pattern of bone contusions is regarded as a footprint, left behind at the site of the injury in the peripheral joint (15), with the mechanism of injury understood by studying the distribution of the edema (15, 16). However, the majority of studies on spinal trauma have been unable to identify any specific pattern in multiple level spinal injury (7, 11, 12). This is probably because the vector forces are multidirectional and it is difficult to designate which injury is a primary lesion, especially when there is a mix of various bone and soft tissue injuries.
We observed certain patterns of subaxial cervical spinal injury, which frequently combined secondary contiguous or non-contiguous subchondral bone contusions. However, we prefer the term "subchondral bone impaction" (SBI) rather than "subchondral bone contusion," as differentiating between a subchondral bone contusion and subchondral compression fractures is difficult in initial imaging studies. Some subchondral compression fractures cause no, or a very subtle, loss in height and new vertebral height loss is only revealed upon follow-up imaging. The purpose of our study was to evaluate the incidence of secondary contiguous or non-contiguous SBIs in subaxial cervical spinal injury and to elucidate the associated primary injury patterns.
MATERIALS AND METHODS
Study population
This study was approved by our institutional review board. The requirement for informed consent was waived for this retrospective study. Between January 2007 and December 2011, 81 patients visited the emergency department of our hospital describing acute neck pain after trauma. Among them, 72 consecutive patients who had an MRI scan and a multidetector computed tomography (MDCT) scan within 72 hours had their images retrospectively reviewed by a neuroradiologist with 10 years of experience.
Patient inclusion criteria were as follows
1) Patients who had a recent fracture representing sharp cortical disruption, as seen in a CT scan, and bone marrow edema seen on a MRI scan of the subaxial cervical spine or cervicothoracic junction.
2) Patients who had acute soft tissue injury to the subaxial cervical spine or cervicothoracic junction, such as that seen as abnormal signal intensity or discontinuity of paraspinal soft tissue including the disc, ligament, or paraspinal muscles/prevertebral soft tissue on a MRI scan.
3) Patients who had abnormal alignment, widening of interspinous space, and widening of the disc space of the subaxial cervical spine or cervicothoracic junction related to a recent fracture or acute paraspinal soft tissue injury.
Patient exclusion criteria were as follows
1) Patients who showed no abnormal finding either in bone or soft tissue of the subaxial cervical spine as seen by CT and MRI.
2) Patients who had combined cervical and lumbar spinal injury, cervical and mid thoracic injury, and atlantoaxial and subaxial cervical spinal injuries were excluded because we wanted to focus on the injury in the subaxial cervical spine and cervicothoracic junction. Patients who had atlantoaxial cervical injury were also excluded for the same reason.
3) Patients who had underlying vertebral morphologic abnormality due to prior surgery, congenital anomaly, prior trauma, bridging ossifications along the anterior longitudinal ligament and posterior longitudinal ligament, or vertebral body fusion by marginal syndesmophytes (bamboo spine) were excluded because these abnormalities can modify the biomechanics of an injury.
According to these criteria, 13 patients with no abnormal findings in the subaxial cervical spine were excluded. Twelve patients who had a prior cervical spinal surgery (n=1), post-traumatic deformity (n=1), congenital block vertebra (n=5), coexistent other thoracolumbar injury (n=2), and C1/2 injury (n=3) were also excluded. Finally, 47 patients (43 males, age range 16-74 years, mean age 46.56 years; and 4 females, age range 33-77 years, mean age 64 years) were enrolled in the study.
Image Acquisition
1) MRI
All MR images were obtained by one of two 1.5T MR machines (Signa HDx, Signa Excite, GE Medical Systems, Milwaukee, Wisconsin, USA). Forty-one patients (41/47, 87.23%) underwent contrast enhanced MRI and 6 patients (6/47, 12.76%) underwent noncontrast enhanced MRI, according to the clinician's preference. Table 1 summarizes the MRI protocols. Contrast enhanced MRI was initiated within 30 seconds of the contrast medium injection using Gadodiamide (Omniscan, 0.2 mmol/kg, GE Healthcare, Princeton, NJ, USA).
2) CT
Unenhanced CT of the cervical spine was performed with a 16-section scanner (Sensation 16, Siemens, Forcheim, Germany) or a 64-section scanner (Lightspeed VCT, GE Medical Systems, Milwaukee, Wisconsin, USA). The unenhanced axial CT examinations were performed with the following parameters, a tube voltage of 120 kVp, use of an automatic dose adaptation system provided by the manufacturer (Caredose, Siemens and AutomA, GE Medical Systems), and a section thickness of 2.5 mm. Coronal, axial, and sagittal reformation was carried out using a 2 mm section thickness.
Image analysis
Two musculoskeletal radiologists with 6 and 20 years experience reviewed the MRI scans and CT scans for consensus. Imaging analyses were done in two steps. The first step was the evaluation of the primary injury patterns of the subaxial spine in all patients, followed by an evaluation of the presence or absence and injury pattern of contiguous or non-contiguous secondary SBI.
To evaluate the primary injury patterns of the subaxial cervical spine, we analyzed the number and level of the primary injury sites, the injury morphology, anterior discoligamentous complex (ADC) injury, posterior discoligamentous complex (PDC) injury, posterior ligamentous complex (PLC) injury, including ligamentum flavum, facet joint, interspinous, ligamentum nuchae, and spinal cord abnormalities. Injury morphology was classified as compression, burst, distraction, or rotation/translation using the subaxial cervical spine injury classification system (SLIC) (17, 18). Compression is defined as a loss of height in the anterior column or in a laminar fracture. A burst is defined as a more severe compression injury that involves the entire vertebral body. A distraction is an anatomic dissociation of the motion segment in the vertical axis, such as a facet subluxation or dislocation, while a rotation/translation is defined as any horizontal displacement of one part of the subaxial cervical spine with respect to the other (17, 18). Additionally, fractures in the spinous process and laminae were classified as compression, except for a Clay Shoveler's fracture, which was classified as a distraction. An ADC injury was defined as the presence of prevertebral soft tissue swelling, with or without high signal intensity of the anterior portion of the discovertebral junction (19). A PDC injury was defined as an irregular herniated disc with high signal intensity, presenting acute disc herniation, or discontinuity of low signal intensity of the posterior annulus/posterior longitudinal ligament complex. A PLC injury was categorized as a suspicious injury or a definite injury. A suspicious injury was defined as having only a signal abnormality of one posterior ligamentous complex. A definite injury required a signal abnormality of more than one of the posterior ligamentous complex structures or one of following findings: 1) a discontinuity of ligamentum flavum due to translation, 2) a facet joint subluxation or dislocation, 3) a spinous process fracture with an abnormal signal intensity of the interspinous, ligamentum nuchae, 4) a widening of the interspinous space, or 5) a definite fluid signal intensity gap in the interspinous, ligamentum nuchae. A spinal cord injury was defined as showing a high signal intensity on the T2 axial and sagittal images, which indicates edema or contusion, and by signal changes that are indicative of hemorrhage or cord infarct (20).
As a second step, the secondary SBIs, which had developed at vertebra contiguous or non-contiguous to the primary injured site, were documented for the presence or absence, number, level, and site (near the superior/inferior endplate, posterior element). Subchondral impactions were defined as geographic, crescentic, diffuse, or linear high signal intensities at the subchondral area on short tau inversion recovery (STIR) images, or contrast enhanced fat suppressed T1 weighted images, suggesting subchondral bone contusions or subchondral compression fractures (21).
Medical records were reviewed by one senior resident for the mechanism of injury (MOI) of all enrolled patients. We considered high-speed motor vehicle accidents (MVAs), strikes by pedestrians/bicyclists, falls from heights or stairs, and high-force direct blows to the head or neck as high-impact MOIs, and hangings/strangulations, low speed MVAs, and falls from standing as low-impact MOIs (22). Treatment was also classified into conservative treatment or operation. When a patient underwent an operation, whether the operation was performed only on the site of primary injury or on both primary and secondary injury sites were documented.
Statistical analysis
Descriptive analyses were carried out for all analyzed factors. Differences in the number of injured vertebrae between patients with and without secondary SBI, and between contiguous and non-contiguous SBI, were tested using the Mann-Whitney U test. Differences in the primary subaxial cervical spinal injury patterns (level, injury morphology, ADC /PDC injury, PLC injury, and spinal cord abnormality), and MOI between patients with and without secondary SBI and between contiguous and non-contiguous SBI, were analyzed using Pearson's chi square test and Fisher's exact test. All of the statistical analyses were conducted using a SPSS 19.0.1 software package (SPSS, Chicago, IL). Differences were defined as statistically significant when P values were below 0.05.
RESULTS
Results of imaging analysis
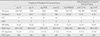
Primary subaxial spinal injury was observed in a total of 94 vertebrae of 47 patients (Fig. 1). Among them, secondary SBI developed in 41 injured vertebrae of 18 patients (18/47, 38.29%), composed of contiguous (n=9) or non-contiguous (n=9) SBI. The SBI were most commonly involving T3 (15/47, 31.91%, Fig. 2) and 3 levels (6/18, 33.33%). All SBIs had developed near the anterosuperior region of the body and the superior endplate. Table 2 shows the results of the statistical analyses of the difference in the number of injured vertebrae at the primary injury site, the primary injury pattern, and the mechanism of injury (MOI) between patients with and without SBI in subaxial cervical spinal injury. SBI was significantly correlated with injury morphology (P=0.001) and most commonly accompanied a rotation/translation injury (10/18, 55.55%). SBI also frequently accompanied PLC injuries with statistical significance (P=0.009), especially, with regard to definite PLC injury (17/18, 94.45%). However, other factors did not yield any statistically significant association (P<0.05).
In terms of contiguous versus non-contiguous SBI, contiguous SBI developed in 26 vertebrae of 9 patients (9/18, 50%) and non-contiguous SBI developed in 21 vertebrae of 9 patients (9/18, 50%). There is a statistically significant difference in the level of primary injury site between contiguous and non-contiguous SBI (P=0.009, Fig. 3). The non-contiguous SBI occurred at a relatively high level of cervical spinal injury (C3-C7) compared to the contiguous SBI, which tended to develop at a relatively low level of cervical injury and cervicothoracic junctional injury (C4-T2) (Fig. 3). Table 3 shows the results of statistical analyses of the difference in the number of vertebrae with secondary SBI, the number of injured vertebrae at the primary injury site, the primary injury pattern, and the mechanism of injury (MOI) between patients with non-contiguous or contiguous SBI in subaxial cervical spinal injury. PDC injuries more frequently accompanied non-contiguous SBI than contiguous SBI, with statistical significance (P=0.009, Table 3, Figs. 4 and 5). All patients (9/9, 100%) in the non-contiguous SBI group sustained PDC injury, while only three of nine patients (33.33%) with contiguous SBI did. Although there was no statistical significance, rotation/translation injuries of the primary injury site more frequently accompanied non-contiguous SBI compared to contiguous SBI. There was no statistically significant difference in other analyzed factors between contiguous and non-contiguous SBI (Table 3).
Results of the review of medical records
In all patients with subaxial cervical spinal injuries, high speed MVAs (17/47, 36.17%) were the most common MOI, followed by falls from heights (9/47, 19.14%), high-force blows (7/47, 14.89%), falls from stairs (5/47, 10.63%), other blunt trauma (3/47, 6.38%), low speed MVAs, falls from standing, and strikes from pedestrians/bicyclists (2/47, 4.25%). Overall, high-impact MOI (40/47, 85.1%) was more common than low-impact MOI (7/47, 14.9%). There was a significant difference in MOI between subaxial cervical injuries with and without secondary SBI (P=0.005, Table 2). All contiguous and non-contiguous SBIs in subaxial cervical spinal injuries occurred due to high-impact MOI (Table 3).
Thirty-six patients (36/47, 76.59%) were treated by operation. Seventeen patients had an anterior interbody fusion (17/36, 47.22%), eight had a posterior fusion (8/36, 22.22%), and five patients had combined operations with anterior and posterior (5/36, 13.88%). Four patients had an anterior interbody fusion with corpectomy (4/36, 11.11%) and one patient had a decompressive laminectomy and laminoplasty (1/36, 2.77%). All patients with non-contiguous SBI (9/9, 100%) had operations and all these operations were at the primary injury site only, not the vertebrae of non-contiguous SBI. Seven of nine patients (7/9, 77.78%) with contiguous SBI had operations. Among them, four patients had operations on the primary injury site only and three patients were operated on for both the primary injury site and contiguous SBI. Among these three patients, one patient who had a distraction injury at C5-7 with contiguous SBI from T1 to T4 received an anterior interbody fusion from C6 to T1. One other patient, who had a burst injury at C5-6 with contiguous SBI from C7 to T3, had a posterior fusion from C5 to C7. Another patient, who had a burst injury at C6-7 with contiguous subchondral bone injury at T1, underwent a posterior fusion from C3 to T3.
DISCUSSION
Secondary SBI at contiguous or non-contiguous vertebrae was found in about 38% of subaxial cervical spinal injuries in this study. Both contiguous and non-contiguous SBI had equally developed and involved multi-levels of vertebral bodies. Our study corresponds with that of Qaiyum et al. (12), which showed that 43% of unsuspected injuries, composed of 12 contiguous and 14 non-contiguous, were revealed by MRI. Choi et al. (23) reported that 28% of patients with cervical spinal injuries had associated non-contiguous spinal injuries. Our study showed a relatively lower incidence (19.15%) of non-contiguous SBI compared to their study. However, their study included not only SBI but also ligament injuries, disc herniations, and spinal cord injuries (23). The broad inclusion criteria of their study may have increased the incidence of non-contiguous spinal injuries compared to our study.
Gupta and El Masri (7) found that multi-level injuries observed on radiographs most commonly involved lower cervical and cervicothoracic levels, which corresponds with our results. In particular, we found that the SBI developed near the superior endplate and occurred at C7 and in the upper thoracic spine (T1 to T5). The cervicothoracic junction forms a gradual transition from lordosis in the cervical spine to kyphosis in the thoracic spine and has coupled movement of side bending and axial rotation with the cervical spine (24). This area is also a transition zone from the flexible cervical spine to the stiff mid to lower thoracic spine. Due to the change in alignment from lordosis to kyphosis, and the relative stiffness of the upper thoracic spine, in our opinion, the high energy compressive force caused by a wide range of flexion-extension motion in subaxial cervical trauma might injure upper thoracic vertebral bodies near the superior endplate and the anterosuperior corner.
All contiguous and non-contiguous SBI of subaxial cervical spinal injuries had developed due to high-impact MOI, with statistical significance. The most common injury morphology of primary sites was rotation/translation, followed by burst and compression. PLC injury was also significantly higher in patients with SBI than without. In contrast, ADC injury was more common in patients without SBI than those with SBI, although there was no statistical significance. Our results suggest high energy compressive flexion forces may result in secondary SBI at either contiguous or non-contiguous levels from the primary injury site, rather than the distractive forces. According to previous studies, there is no clear correlation between the pattern of multi-level spinal injury and the mechanism of injury. There are a number of reasons why our results disagree with the findings of previous studies. Firstly, many of the previous studies included various secondary spinal injuries, such as bone contusions, fractures, ligamentous injuries, and traumatic disc herniations, in contrast to our study in which we focused on SBI. Secondly, they included multi-level injuries in whole spines, which can affect multidirectional vector force. Thirdly, in the study by Choi et al. (23), the cervical spinal injuries were classified according to the Allen and Ferguson classification system (25), while we classified according to the SLIC scoring system. The Allen and Ferguson classification system (25) is based on mechanical details but its complexity means that intra-class correlation is low (18). Hence, we used the more simplistic SLIC classification system (18) to more easily and reliably classify injury morphology.
There are a number of differences between contiguous and non-contiguous secondary SBI. Non-contiguous SBI developed in the upper levels of the primary injury site (C3-C7) compared to contiguous SBI (C4-T2) and was more frequently accompanied by PDC injury at the primary injury site, with statistical significance. Although there was no statistical significance, rotation/translation injuries of the primary injury site more frequently accompanied non-contiguous SBI compared to contiguous SBI. These results suggest that non-contiguous SBI of subaxial cervical spinal injuries are more likely to have a close relationship with high energy flexion forces. These forces injure both ligaments in the posterior portion of the discovertebral junction and posterior arch at a relatively high level of the cervical spine compared to contiguous SBI.
In our study, the majority of operations was performed only for the primary injury site and did not involve SBI. Previous studies have reported that the second injury had no important bearing on management, and that the prognosis for multi-level spinal fracture was not significantly worse than that for single-level fractures. This is probably because the secondary lesion was most commonly a bone contusion. Although we presume that SBIs of the spine are self-limiting, benign abnormalities, further evaluation with short term and long term follow-up is required.
The limitations of this study stemmed, first and foremost, from the retrospective nature of the analysis. All primary cervical spinal injuries and SBIs were diagnosed by image modalities and not by surgery or pathology. A previous study (26) reported that MRI is sensitive (67-100%) for the evaluation of PLC injury in acute cervical trauma, but has a lower positive predictive value (42-82%) and specificity (56-67%). Therefore, there is a possibility of over-read of PLC injury by MRI in our study. Moreover, we did not evaluate the confidence level and interobserver/intraobserver agreement of the diagnosis of ADC, PDC, and PLC injury. We suggested that SBI could predict the injury mechanism, but we used the SLIC scoring system (18), which is based on the morphology of injury, instead of the Allen and Ferguson classification system (25), which is based on mechanism of injury.
Apart from these limitations, our study has several clinical significances. Firstly, we proved that the secondary SBI of subaxial cervical spinal injuries are not infrequent and could develop into either contiguous or non-contiguous levels. Although the SBI usually did not include the operation level, it could be a source of pain. Careful evaluations of SBI in contiguous and non-contiguous levels from the primary site are needed, especially in certain types of morphology of subaxial cervical spinal injuries. Secondly, the result that most SBI had developed from C7 to T5 vertebrae can help to elucidate the biomechanics between the subaxial spine and the upper thoracic spine. Thirdly, our study proves that high energy compressive flexion forces of the subaxial cervical spine can be associated with both contiguous and non-contiguous levels of SBI, although it is more likely associated with non-contiguous SBI. Our results also help in understanding and explaining the biomechanics of subaxial cervical spinal injuries, which differ from thoracic and lumbar spinal injuries. In conclusion, regarding subaxial cervical spinal injuries, secondary SBI is common and is probably associated with injury by high energy compressive flexion forces.







 XML Download
XML Download