

 PDF
PDF ePub
ePub Citation
Citation Print
Print


INTRODUCTION
Intramedullary spinal lesions in the conus medullaris (CM), including tumors, infection and vascular lesion, are rarely reported. Intramedullary spinal cord tumors account for 1% of all central nervous system tumors (1) and some infectious diseases in the CM were reported as case reports (2, 3, 4, 5, 6, 7, 8, 9, 10). Moreover some authors described syringomyelia of the CM due to spinal arteriovenous malformation (11). In a previous literature, 26.8% of 447 ependymomas were commonly located in the CM (12). Although they had a nonspecific radiologic appearance, Kim et al. (13) suggested some diagnostic clues of ependymoma were central location, diffuse enhancement, syringomyelia, hemorrhage and cap sign using MR imaging.
MR imaging is currently used as an imaging modality of choice in defining intramedullary spinal cord lesions (14, 15). MR imaging of the spinal cord tumor includes evaluation of tumor characteristics, the extent of cord involvement, enhancement pattern (14, 16).
Therefore we reported various MR features of intramedullary spinal cord involving the CM in six patients and tried to discuss them for differential diagnosis.
MATERIALS AND METHODS
This retrospective study was approved by our institutional review board and the requirement for the informed consent was waived. Six patients (male: female = 4:2, mean age = 44.3 year old) were enrolled from the clinical database of our institute from 2004 to 2010 and their radiological images and clinical symptoms were reviewed retrospectively. Intramedul-lary CM tumor was defined as the primary spinal cord tumor involved only at CM. Pathology was confirmed in five patients after total surgical resection (Table 1).
All patients had taken initial and postoperative MRI with contrast enhancement using gadopentate dimeglumine (Gd-DTPA). Lumbar-sacral MR imaging was performed using 1.5-T system (Vision 1.5T and Avanto 1.5T; Simens medical systems, Erlangen, Germany). Axial and sagittal T1, T2-weighted fast spin-echo sequence and contrast enhanced T1-weighted images were taken in 1.5-T system (T1WI: TR/TE=560/9.8 msec; number of sections, 17; section thickness, 3 mm; field of view, 35 cm; matrix, 314 × 448; number of signals acquired, two; echo train length, 3; and voxel resolution, 1.1 × 0.8 × 3.0 mm, T2WI: TR/TE=3760/100 msec; number of sections, 17; section thickness, 3 mm; field of view, 35 cm; matrix, 338 × 512; number of signals acquired, four; echo train length, 3; and voxel resolution, ; 1.0 × 0.7 × 3.0 mm). These images were reviewed independently by two experienced neuroradiologists (S.J.A, T. S.C) and analyzed by the following parameters; tumor size, location, signal intensity relative to the spinal cord, vascular flow voids, syrinx or cyst, edema and enhancement pattern.
RESULTS
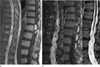
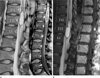
Six intramedullary spinal masses were located from the 12th level of the thoracic vertebra to the 2nd level of the lumbar vertebra and their size varied from 21 to 62 mm (Table 1). Three cystic masses were intermingled with the solid portion, which showed variable signal intensities on T1 weighted (T1WI) and T2-weighted images (T2WI) (Figs. 1, 3). Two purely cystic lesions showed the same signal as the cerebrospinal fluid (CSF) (Fig. 2). Contrast enhancement was seen in all intramedul-lary masses. An eccentric enhancing nodule was noted in two hemangioblastomas (Figs. 1a, 2b) and unusual peripheral rim enhancement with septation was seen in ventriculus terminalis (Fig. 2a). Patchy enhancement of the CM was observed in spinal arteriovenous fistula (AVF) (Fig. 1b). Extensive cord edema and hydrosyrinx was seen adjacent to the intramedullary lesions in three cases. Vascular signal voids were found in two hemangioblastomas and one spinal AVF which were confirmed as "dilated medullary vein" on spinal angiography. On the follow-up two cases (patient 1 and 2), which showed residual or recurrent contrast-MR imaging, four cases showed almost complete resolution after total surgical resection or embolization and enhancing lesions two years after surgery.
Spinal angiography was performed in three patients to evaluate preoperative embolization of two hemangioblastomas and one AVF and transarterial embolization was performed in the latter.
Five patients had frequent lower back pain, combined with leg pain in two and buttock pain in one. Urinary disturbance was seen in two patients. In spinal AVF, sudden-onset weakness in extremities and sensory change was noted. All patients improved their symptoms after operation or embolization.
DISCUSSION
We described six different cases of intramedullary spinal pathologies involving the CM, including ependymoma, hemangioblastomas, dermoid cyst, ventriculus terminalis and spinal AVF. Irrespective of tissue pathology, intramedullary lesions involving the CM had some MR imaging in common; 1) relatively larger mass, more than 20 mm with swelling of the CM, 2) contrast enhancement of the solid component, 3) central location on the CM except one hemangioblastoma. The unusual MR features in this study were syringomyelia and patch cord enhancement in spinal AVF, cystic wall enhancement with an internal septum in the ventriculus terminalis and peripheral rim enhancement of the dermoid cyst.
Tumor size of our five cases involving the CM was relatively large, more than 20 mm. Epstein et al. (17) suggested dominant motor symptoms were commonly associated with very large ependymomas and a poorer postoperative outcome secondary to the increased surgical risk. Although swelling of the CM was found, hydrosyrinx occurred in only three cases, two cases of which were combined with extensive cord edema and dilated medullary vein. The cause of syrinx and cord edema may be associated with intramedul-lary cord tumor as well as venous hypertension. While the syrinx was frequently reported in 9-50% of ependymoma (16, 18) and 40-81% of hemangioblastoma (19, 20, 21, 22), the syrinx was a rare pathology in case of spinal AVF. Srivatanakul et al. (11) reported that venous hypertension in the spinal cord was the trigger for the development of syringomyelia and showed disappearance of syrinx after transarterial embolization.
Typical MR imaging of spinal ependymomas usually show isointensity or slightly hypointensity on unenhanced T1-weighted images (15, 18, 23, 24). Ependymomas show hyperintencity in rare occasions, when the myxopapillary ependymoma is associated with hemorrhage or mucin production (18, 23). After gadolinium enhancement, lesions show homogenous, heterogenous or only rim enhancement (15, 18, 23, 24). About 20% of cases of ependymomas can show low signal intensity rim on T2-weighted images, which indicates the presence of hemosiderin deposit (23). Combined nontumoral cysts are common in about 78-84% ependymomas and incidence of tumoral cysts are about 4-50%, which is variable (16, 18, 23). Syringomyelia were variably associated in about 34-90% of ependymomas (18, 25). Our one case of ependymomas also showed cystic portion, which is also probably related to hemorrhage or necrosis.
Spinal hemangioblastomas shows hypointense to isointense on T1WI and isointense to hyperintense on T2WI (20, 26, 27, 28). On T2WI, hemangioblastomas can have intermixed focal flow voids (20, 26, 27, 28). Cyst formation or syringohydromyelia is very common (19, 20, 22, 26, 29) like our two cases. Our two cases of hemangioblastomas showed mostly cystic lesions with eccentric enhancing nodules which was compatible with typical MR findings of the previous studies (26, 28, 30). Both cases showed extensive cord edema and flow-void signal within the lesion.
The ventriculus terminalis is a round cystic cavity with smooth wall, no internal septa and no contrast enhancement of the cyst or its wall (31, 32, 33, 34, 35, 36, 37, 38). However, there was an internal septation and cystic wall enhancement in our case, which would lead to surgical resection because of misdiagnosis as spinal astrocytoma. Cystic wall enhancement was likely to be originated from venous hypertension or combined inflammatory change.
Spinal dermoid cysts showed usually hyperintensity on T1WI due to fatty secretion of sebaceous gland and cholesterol and usually hypointensity on T2WI but might be homogenous or heterogenous (39, 40). Spinal dermoid cysts did not usually enhance on postcontrast examination (3, 41). However our case showed heterogeneous intensity in T1 and T2WI as well as peripheral enhancement of the solid component (Fig. 3b). Enhancement of spinal dermoid cysts was a rare entity; only two cases were reported that was peripherally enhanced (42, 43).
Typical MR imaging of dural AVF show increased signal intensity on T2WI throughout the central area of the cord, particularly at CM and decreased signal intensity on T1WI. Prominent signal voids are frequently associated in subarachnoid space, which are the result of dilated vein. Spinal angiography provides the exact location and size of a lesion and information about feeding and draining vessels. Our case showed mostly cystic lesion with expansive cord edema and focal enhancement, probably due to chronic ischemic insult.
In conclusion, although this study had some limitation of heterogeneity and small numbers, intramedullary spinal pathologies of the CM have typical MR characteristics as well as some exceptional imaging features. In evaluation of intramedullary spinal lesions in the CM, it is necessary to consider these unusual MR findings and discriminate various pathologies with prudence and caution.


 XML Download
XML Download