

 PDF
PDF ePub
ePub Citation
Citation Print
Print


INTRODUCTION
Although the overall survival of women that received breast conserving therapy (BCT) and radiation therapy is equivalent to that of mastectomy (1, 2, 3,4, 5), failure to maintain local control is clearly associated with a reduction in long-term cancer-specific survival (6). Negative surgical margin of resection at the time of BCT for breast cancer is associated with substantially lower recurrence rates (7). In previous studies, various factors, including age, tumor size, and pathologic contents, have been evaluated with regard to the re-excision rate (8, 9, 10, 11, 12, 13, 14, 15).
Breast magnetic resonance imaging (MRI) has become a frequently employed imaging modality in the evaluation of the local extent of disease in patients with a confirmed diagnosis of breast cancer. The sensitivity of breast MRI is close to 100% in the context of preoperative evaluation. This high sensitivity is presumed to improve the selection of patients for BCT and reduce the rates of re-excision. MRI detects additional foci of disease in the ipsilateral breast of patients with known breast cancer in 10-30% of cases (16). Clinically and mammographically occult cancer in the contralateral breast is detected in 3-5% of patients who undergo preoperative breast MRI (16). Furthermore, several studies have shown alterations in surgical management planning in approximately 20-30% of all breast cancer patients undergoing preoperative MRI, with an associated increase in mastectomy rates (8, 11, 12, 13, 15). Concerns have been raised that such false-positive findings may increase the use of mastectomy without any clear survival benefit. In a previous study, no significant difference was observed in the recurrence rates between the patients who underwent preoperative MRI versus those who did not. Additionally, low rates of recurrence after both BCT and mastectomy were reported (14, 17). Therefore, the role of preoperative MRI in breast cancer patients being considered for BCT remains a matter of some controversy.
However, preoperative breast MRI has been routinely performed in certain institutions; breast MRI remains a relevant surgical planning tool. Therefore, it is necessary to determine which preoperative MRI findings are associated with re-excision. The objective of this study was to determine the MRI features associated with immediate further surgery due to the presence of a positive margin after BCT in breast cancer patients.
MATERIALS AND METHODS
Patients and Lesions
This study was approved by the institutional review board, which waived the requirement for informed consent. At our institute, all patients with biopsy results indicating breast cancer underwent preoperative MRI. The patients' medical records were reviewed in order to obtain patients' information and MRI findings. We retrospectively evaluated 443 consecutive newly diagnosed breast cancer patients from January 2006 through December 2007. Among these, 286 (65%) cases underwent conservation surgery. Among these 286 cases, 40 were excluded: 20 cases in which no preoperative MRI study data were available, and 20 cases involving preoperative systemic therapy. Thus, a total of 246 BCT cases of 241 patients (mean age, 49 years; range, 25-84) were ultimately included in our study, and of these, 236 patients received unilateral conservation surgery and 5 patients received bilateral conservation surgery.
Surgical Therapy
All conservation surgeries were conducted by a single surgeon (S.W.K) with 9 years of experience in breast cancer surgery. Conserving surgery was suggested for the majority of women with stage I or II early breast cancer or with a maximum cancer diameter of less than 4 cm after review of all imaging data, including MRI data (2, 18). The expected percentage of residual breast volume after wide excision and the patient's preferences were also considered. Subareolar tumors (23 cases) were approached by central excision with or without resection of the nipple areolar complex depending on the tumor involvement. Palpable tumors (152 cases) were excised with the acceptable margin width of more than 1 cm by intraoperative palpation without any image guidance. Non-palpable malignant lesions (94 cases) were routinely guided by breast radiologists using ultrasound- or mammography-guided hookwire needle localization. Ultrasound-guided needle localization was performed in 77 cases and mammography-guided needle localization was performed in 17 cases. In some cases with non-palpable tumors, specimen mammography was performed to confirm adequate resection. Intraoperative frozen sections for evaluation of the resection margins were not routinely collected. Pathology reports included size, histologic grade, and surgical margin status. Margins were classified as involved (positive) or clear. Involved margins were defined as those with tumor cells less than 2 mm from the inked margin in invasive breast cancer, and less than 1 mm from the inked margin in ductal carcinoma in situ (DCIS). Patients with involved margins were expected to undergo further surgery within 2 weeks. If the residual volume was sufficient and the patients desired a re-trial, they underwent another wide local excision rather than a mastectomy.
MRI sequence
All MRI examinations were conducted using 1.5 T or 3.0 T magnets (1.5 T Intera and 3.0 T Achieva, Philips Healthcare, Best, Hamburg, Germany), randomly. Patients were placed in the prone position with both breasts imaged using a one-channel dedicated coil for 1.5 T MRI, and a four-channel dedicated coil for 3.0 T. For 1.5 T MRI, our standard protocol consisted of a transverse T1-weighted localizer sequence through both breasts followed by a fat-saturated sagittal T2-weighted fast spin-echo acquisition (SPAIR) (TR/TE, 2300/65), and a dynamic series consisting of a T1-weighted two dimensional gradient echo pulse sequence (TR/TE, 290/4.6)], and a flip angle of 15° through the affected breast. For the 3.0 T MRI protocol, a transverse T1-weighted localizer sequence through both breasts was followed by a fat-saturated sagittal T2-weighted fast spin-echo acquisition (SPAIR) (TR/TE, 5,000/120), and a dynamic series consisting of a T1-weighted two dimensional gradient echo pulse sequence (TR/TE, 269/2.3), and a flip angle of 12° through the affected breast. Scanning parameters included the typical section thickness, 3-5 mm; the field of view, 26-35 cm depending on patient size; and a matrix of 344 × 345. Axial and coronal reformations, in addition to maximum intensity projection (MIP), were constructed from the first contrast-enhanced image. Imaging was initiated via a bolus injection of gadodiamide at a dose of 0.1 mmol/kg of body weight (Omniscan, GE healthcare), administered through a needle into the antecubital vein, followed by a 20-mL flushing bolus of isotonic saline solution. The total injection time was 10 seconds. Contrast-enhanced sagittal T1-weighted series were 60 seconds in duration and centered at 60, 120, 180, 240, and 300 seconds for the ipsilateral breast. After contrast-enhanced high-spatial-resolution images and their subtraction images were used for lesion detection, time-intensity plots of diagnosed breast cancer lesion dynamic images were generated using dedicated MRI software.
MRI analysis
MRI review was retrospectively performed by two radiologists (S. M. K., M. J.) with 8 and 5 years' breast MRI experience, by consensus. Bilateral breast MRI was interpreted with the benefit of a brief clinical history, knowledge of the initial histopathologic findings, and knowledge of the mammography and sonography results. However, both radiologists were blinded to the patient's final pathological result and the reports of the initial MRI interpretation. We classified MRI features of breast cancer based on ACR BI-RADS (Breast Imaging and Data Reporting System) MRI lexicon. (19) According to this lexicon, we categorized the lesion type on MRI as mass or non-mass-like enhancement (NMLE). In cases of mass, we additionally categorized kinetic curve delay enhancement characteristics as persistent, plateau, and wash out patterns based on the time-intensity plots of dynamic images. In cases of NMLE, we additionally categorized distribution as linear, ductal, segmental, regional, multiple regional, or diffuse patterns. We included mass associated with adjacent or coexistent NMLE of breast lesion. The shape, margin, internal enhancement of mass, and internal enhancement of NMLE were not included in our additional evaluations. We analyzed the size and number of lesions evident on MRI. Multifocal cancer was defined as the presence of two or more foci of cancer in the same quadrant that were separated by less than 2 cm of normal parenchyma. Multicentric cancer was classified as the presence of two or more foci of breast cancer in different quadrants. In cases of multifocal or multicentric lesions, the lesion size on MRI was determined at the largest portion. We also reviewed the lesion location in terms of distance from the nipple and distance from the chest wall on MIP images.
Data analysis
We analyzed clinical factors such as age, palpability, and breast cancer history with regard to re-excision. We also analyzed the pathologic reports of final surgical specimens according to histologic type and the existence of a DCIS component, and conducted immunohistochemical analyses including hormone receptor and human epidermal growth factor receptor type 2 staining scores. TNM staging was also evaluated based on the sixth American Joint Committee on Cancer (AJCC) guidelines (20).
Statistical analyses were conducted using the χ2 test, Fisher's exact test, and Student's t-test using SPSS version 19.0 for Windows (SPSS Inc., Chicago, IL). We considered p values less than 0.05 to be indicative of a statistically significant difference. Multivariate analysis was performed using logistic regression of the variables that were found to be statistically significant through univariate analysis, and was used to estimate odds ratios (ORs).
RESULTS
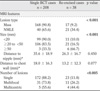
In accordance with our surgical therapy guidelines, 38/246 (15.4%) cases subsequently underwent reexcision. Among these 38 cases, 11 (28.9%) received subsequent total mastectomy and 27 (71.1%) underwent one additional wide local excision. Among these 27 cases, 3 received one further local excision and ultimately underwent total mastectomy. Clinical factors that were not significantly associated with re-excision included age (p = 0.268), palpability (p = 0.591), and breast cancer family history (p = 0.543) (Table 1). We analyzed the final pathologic report of surgical specimens with regard to re-excision. Tumor histology was significantly associated with re-excision (p < 0.001). Additionally, the coexistence of a DCIS component in invasive ductal carcinoma was significantly correlated with re-excision. In cases of pure invasive ductal carcinoma without a DCIS component, only 2.9% (1/34) required re-excision. On the other hand, in cases of invasive ductal carcinoma involving DCIS components, 12.1% (16/132) required re-excision. In cases of pure DCIS, 36.7% (18/49) required re-excision. Twenty percent (2/10) of cases of invasive lobular carcinoma (ILC) required re-excision due to positive surgical margin. No significant correlations were noted between receptor status and re-excision (Table 1).
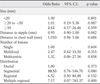
Table 2 compares the group that required immediate re-excision due to the presence of a positive margin (n = 38) and the group in which a single BCT was sufficient (n = 208) according to MRI variables, including the type, size, and location of lesions, and the number of lesions. In cases of mass, re-excisions were conducted in 9.2% (17/185) of the patient group (Fig. 1). In the patients exhibiting NMLE on MRI the rate of re-excision was 34.4% (21/61) (Fig. 2), which was significantly higher than that of patients with masses (p < 0.001). The mean size of malignant lesions was 20.7 ± 9.2 mm (range, 9-65 mm) in single BCT cases and 29.6 ± 15.0 mm (range, 5-59 mm) in cases involving re-excision. Lesion size was positively associated with re-excision (p < 0.001). The distance from the nipple and chest wall, i.e., the lesion location, was not significantly associated with re-excision. Multiplicity of cancer identified via MRI was significantly associated with re-excision (p = 0.003) (Fig. 3). Among 61 cases exhibiting an MRI pattern indicative of NMLE, the distribution was significantly associated with reexcision (p = 0.047). In 30 NMLE cases in which segmental distribution was observed, 50% (15/30) underwent re-excision (Fig. 2) (Table 3).
In multivariate logistic regression, larger size, NMLE pattern, and multiplicity on MRI were significantly associated with re-excision (Table 4). With regard to those significant MRI factors, size larger than 5 cm (OR = 3.81), NMLE type (OR = 2.96), and multifocal lesion (OR = 2.96) were independently predictive of re-excision. Among the NMLE lesions, additional multivariate logistic regression analysis was performed incorporating all variables associated with re-excision. NMLE with segmental distribution was strongly associated with re-excision (OR =10.53) (Table 5).
DISCUSSION
With regard to breast cancer, it is well known that involved surgical margins are associated with higher local recurrence rates, (21, 22, 23) and in a recent meta-analysis, increased local recurrence was associated with poorer overall survival (6). Negative surgical margin in women undergoing BCT is universally accepted as a standard method of reducing the risk of local recurrence (24, 25). In some previous studies, the rates of margin-positive resection remain within a range of 20-70% (7, 10, 24). Additionally, re-excision after BCT is associated with increased expense, compromised cosmesis, patient anxiety, and delays in adjuvant therapy, and it can also be associated with compromised oncologic outcomes (26, 27, 28).
In this study, we conducted breast cancer treatment according to the NCCN practice guidelines (24). Usually, conservation therapy of the breast is associated with tumor size, extent, expected residual volume, and patient preference. Owing to the development of surgical techniques using skin flaps and nipple reconstruction, we can now attempt BCT more often in locally advanced cases. As compared to rates reported in previous studies, (26, 29, 30, 31, 32, 33) the overall re-excision rate of 15.4% (38/246) in this study was relatively low.
In previous studies, larger size, ILC, and the presence of DCIS (either as the principal pathology or in association with invasive cancer) were the factors that were the most consistently associated with margin positivity (26, 29, 30, 31, 32, 33, 34). Younger age, high nuclear grade, and the presence of lymphovascular invasion have also been associated with a higher rate of margin positivity (26, 29, 30, 32, 33, 34, 35, 36). In our study, clinical factors including age, family history, and personal history of breast cancer were not significantly associated with re-excision. ILC is slow-growing, and as it grows, it fails to invoke a desmoplastic reaction. Unique histology of ILC can be the cause of detection difficulty, both clinically and radiographically. ILC is reportedly associated with higher rates of positive margins at excision than invasive ductal carcinomas, (37, 38) especially without preoperative MRI (39). In our study, 2/10 (20%) re-excised patients with ILC were treated with BCS. These results were within the range of the previously reported rates of 15.8% (29) and 51% (34). In our study, the presence of a DCIS component was significantly associated with re-excision. This result substantiated the findings of previous reports (26, 29, 30, 31, 32, 33, 34) that the DCIS component is significantly associated with the presence of a positive margin. In 49 cases of DCIS only, 18 (36.7%) underwent re-excision.
In this study, the MRI factors that influenced the re-excision rate were lesion size, number of lesions, and NMLE type, particularly segmental distribution. Associations between re-excision and multiplicity of lesions and larger tumor size have been studied previously (26, 31, 40, 41). A review of the correlation between MRI-determined tumor size and pathologically determined tumor size is imperative. MRI tumor size correlates with pathologically determined size; however, significant overestimation occurs in cases where both invasive and non-invasive tumors are present (42). In our study, tumor staging on final pathology was associated with re-excision (p = 0.045). However, this result does not imply a positive correlation. While the re-excision rate was 30.6% (11/25) in Tis patients, the rates were 10.3% and 0% in T2 and T3 respectively. Therefore, tumor size as measured by MRI could predict re-excision because MRI effectively detects DCIS (43). This result also explains the observation that in cases of NMLE with segmental distribution, DCIS is most often apparent, (43) which is associated with a high re-excision rate. NMLE pattern was significantly associated with re-excision in our study. Therefore, NMLE pattern on breast MRI implies a greater likelihood of the presence of a DCIS component or an extensive intraductal component, aside from the pathologically confirmed tumor itself. Moreover, preoperative lesion localization using ultrasound or mammography guidance, not MRI, would be problematic in cases of NMLE lesions. NMLE patterns with multiple regional distributions were also positively associated with re-excision. However, there were only 2 cases of NMLE patterns with multiple regional distribution, limiting the interpretation of it as a risk factor. Lesion multiplicity was identified as a risk factor for re-excision. Of the 42 cases of multifocal lesions, 11 (26.6%) involved re-excision, and 4/9 (44.4%) of the cases of multicentric lesions involved re-excision. If a multiple or multicentric tumor is suspected, careful planning and performance of BCT are always required. Multiple bracketing wires using image-guided localization could make it possible to approach multiple lesions from the perspective of conservation.
The lesion location with regard to the distance to the nipple and chest wall was not significantly associated with re-excision. We did not consider the relationship between the tumor and the nipple or the tumor and the chest wall to be significant factors with regard to decisions relating to conservation or surgical techniques such as central lumpectomy with or without nipple areolar complex, or modified pectoralis muscle approaches. Even in cases with nipple involvement, localized lesions could be excised, as has been previously reported (44, 45).
Our study had some limitations. The total number of re-excision cases was relatively small. Another limitation is selection bias, which is inherent in any retrospective study. We focused on the outcomes of patients who underwent BCT, and this could have influenced the results of the study. We have utilized 1 channel or 4 channel coil. Low channel number of receiver coil may affect the signal to noise ratio and reduce the quality of signal. Additionally, we used two different magnetic resonance systems randomly.
In this study, larger size, lesion multiplicity, and the presence of an NMLE pattern on MRI were associated with involved margin. These factors should be considered to ensure proper surgical management and to lower the re-excision rate. BCT can be planned initially even in cases that involve multiple lesions, larger size, and NMLE pattern on MRI. However, when we plan BCT, these findings may prove useful for preoperative patient counseling and may help guide the surgeon in their decision as to whether to perform a wider excision in these patients. Further investigation is required with regard to the MRI factors that are associated with higher rates of re-excision.
In conclusion, larger size, multiplicity, and NMLE on MRI are positively associated with re-excision after BCT in breast cancer patients. In the NMLE lesion type, the segmental distribution pattern is predictive of re-excision.






 XML Download
XML Download