

 PDF
PDF ePub
ePub Citation
Citation Print
Print


INTRODUCTION
MRI is commonly used to evaluate lumbar spine abnormalities in patients with symptoms such as lower back pain, leg pain, paresthesia, weakness in the legs, and claudication. Occasionally, these symptoms are caused by pathologic lesions in the cervical or thoracic spine and mistaken for those caused by lumbar spine lesions. Some pathologic lesions in the cervical or thoracic spine may be serious and need early diagnosis for prompt treatment.
In our hospital, additional cervicothoracic spine sagittal T2-weighted images (CT SAG T2WIs) have been obtained routinely in lumbar spine MRI for eight years. CT SAG T2WIs are easily obtained in short time, about 1 minute 40 seconds, without positional change or additional survey acquisition. According to our experience, CT SAG T2WI is useful for screening a pathologic lesion in the cervical or thoracic spine. However, to the best of our knowledge, there has been no study about the usefulness of CT SAG T2WIs in routine lumbar spine MRI.
The aim of this study was to evaluate usefulness of CT SAG T2WIs included in routine lumbar spine MRI.
MATERIALS AND METHODS
Patients
Institutional review board approval was obtained. Informed consents were not required for this retrospective study. 2,238 patients underwent lumbar spine MRI from January 2005 to December 2005 in our hospital, for their symptoms such as lower back pain, leg pain, paresthesia, weakness in the legs, and claudication. Among 2,238 patient 125 patients were excluded from the study. Exclusion criteria were; (i) the patients with previous cervical or thoracic spine MRI or CT scan or simultaneously with lumbar spine MRI(n = 13); (ii) the patients who were highly suspected to have concurrent pathologic conditions in cervicothoracic spine and practically indicated for cervical or thoracic MRI (e.g. patient with metastasis [n = 57], multilevel lumbar spine compression fracture [n = 40], primary spinal cord/intradural extramedullary tumors [n = 14], or tethered spinal cord in lumbar spine [n = 1]). One radiologist retrospectively reviewed radiologic report of lumbar spine MRI and medical record in 2,113 patients.
Imaging Studies
All MR imaging were obtained with two 1.5-T units (Gyroscan intera, Philips Medical Systems, Best, the Netherlands; Intera, Philips Medical Systems, Best, the Netherlands) by using a five-channel synergy spine coil. In addition to the conventional lumbar spine MRI sequences, sagittal and axial T1- and T2-weighted images, CT SAG T2-weighted spin-echo (SE) sequence (TR/TE, 3000-4000/100; number of signals acquired - 2; matrix size - 512×512; slice thickness - 4 mm; acquisition time - 1 minute 40 seconds) was obtained without positional change by using the same five-channel synergy spine coil.
Imaging Analysis
In 2005, one of four spine radiologists who have eight, six, five and five years of experiences, respectively, interpreted lumbar spine MRI. In May 2011, one radiologist retrospectively reviewed radiologic report for whether pathologic lesion was present or absent on CT SAG T2WIs. In all subjects, radiologist also assessed the following lesions on the radiology report: spinal cord compression associated with spinal stenosis or disc herniation with or without intramedullary T2-high signal intensity (IM-T2-HSI), spinal cord abnormalities (e.g., syrinx, spinal cord atrophy, spinal cord tumors or demyelinating disease, idiopathic spinal cord herniation), vertebral abnormalities (e.g., fracture, anomaly, tumor, or infection), and epidural abnormalities (e.g., hematoma, abscess, or cerebrospinal fluid leakage) in the cervical or thoracic spine. Definitions of these pathologic lesions are in Table 1 (1-4). The radiologist also reviewed record of cervical or thoracic spine MR imaging or CT which were additionally obtained for further evaluation for positive finding on CT SAG T2WIs.
Review of Medical Records
In patients with positive findings on CT SAG T2WIs, medical records were reviewed retrospectively by one radiologist. The radiologist checked interval between initial lumbar spine MRI and additional cervical or thoracic MRI or CT and management of these lesions. Patients' chief complaints were assessed to analyze their correlation between pathologic lesions on CT SAG T2WIs.
RESULTS
Pathologic lesions on CT SAG T2WIs
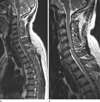
139 (6.58%) of 2,113 patients had 142 pathologic lesions on CT SAG T2WIs (Table 2). Forty of the patients (mean age, 69 years; range, 54-81 years) had concurrent cervical and lumbar spinal stenosis which is called tandem spinal stenosis. Four patients had pathologic lesions only at cervical and/or thoracic spine level on CT SAG T2WIs without any pathologic lesions in the lumbar spine level. One patient who was suspected to have CSF leakage at the lumbar spine level revealed no abnormal finding at lumbar spinal level. But CT SAG T2WIs showed fluid collection in posterior epidural space with CSF leakage and posterior epidural enhancement at upper thoracic spine level (T3-5) (Fig. 1). The other three patients, each of them had spinal canal stenosis and IM-T2-HSI at the level of the C6-7 disc, disc herniation and IMT2-HSI at C4-5 and linear fracture at C7 and T8 in the third.
Further evaluation with cervical or thoracic spine MRI and/or CT for pathologic lesions on CT SAG T2WIs
In 139 patients who had pathologic lesions on CT SAG T2WIs, thirteen patients underwent additional cervical or thoracic spine MRI and/or CT (Table 3). Nine patients underwent MRI of the cervical or thoracic spine. Three patients were performed both MRI and CT. One patient underwent thoracic spine CT. The intervals between lumbar spine MRI and cervical or thoracic spine MRI or CT spanned from one day to 730 days (mean = 123.2 days).
Pathologic lesions were followings: spinal stenosis or disc herniation with definite IM-T2-HSI (n = 6) (Figs. 2 and 3); disc herniation with cord compression but no IM-T2-HSI (n = 1); spinal stenosis resulting from ossification of the posterior longitudinal ligament (OPLL) (n = 1); idiopathic spinal cord herniation (n = 2) (Fig. 4); ankylosis of vertebral bodies resulting from tuberculous spondylitis (n = 1); CSF leakage in spontaneous intracranial hypotension (n = 1) (Fig. 1); and compression fracture (n = 1). Diagnoses of these pathologic lesions were consistent with CT SAG T2WI findings except for one patient initially reported as thoracic spinal cord angulation, who diagnosed as idiopathic spinal cord herniation after her thoracic spine MRI.
Treatment for pathologic lesions on additional CT SAG T2WIs
Seven of 139 patients who had pathologic lesions on CT SAG T2WIs with correlated symptom underwent surgery for their lesions in cervical or thoracic spine. One of the patients who had spinal canal stenosis and IM-T2-HSI at the level of C5-6 on CT SAG T2WIs underwent surgical treatment in 82 days after initial lumbar spine MRI without additional cervical spine MRI or CT scan. In other six patients, either cervical/thoracic MRI or CT scans were performed for further evaluation of pathologic lesions on CT SAG T2WIs before the surgery. Then, they underwent surgery within 90 days (mean: 19.83 days) after their cervical or thoracic MRI or CT scans. Their symptoms were improved after their surgical treatment. The pathologic lesions on CT SAG T2WIs, symptoms of the patient, the management and outcome of these lesions are described in Table 3.
DISCUSSION
Among 2,113 patients, 139 (6.58%) had 142 pathologic lesions on CT SAG T2WIs. The most common pathologic lesions found on CT SAG T2WIs in this study were spinal stenosis or disc herniation with or without IM-T2-HSI (n = 118, 85%). In 139 patients who had pathologic lesions on CT SAG T2WIs, thirteen patients underwent additional cervical or thoracic spine MR imaging and/or CT for confirmative diagnosis and management planning. Six of the thirteen patients underwent surgical treatment. Besides, one patient underwent surgery without additional cervical spine MRI or CT scan.
Spinal canal stenosis, the most common pathologic lesion in this study, can occur in any level; however, it presents most commonly in cervical and lumbar spines. Cervical spinal stenosis may coexist with lumbar spinal stenosis, a condition that is called tandem spinal stenosis. Tandem spinal stenosis has a reported prevalence rate of 5-25% (5-7). In tandem spinal stenosis, the symptoms of either the cervical or the lumbar type can overlap in such a way that the symptoms caused by cervical myelopathy might erroneously be deemed symptoms of lumbar spinal stenosis. Therefore, patients with symptom of severe lumbar spinal stenosis should be evaluated for the presence of cervical myelopathy (5, 8). In our study, out of 139 patients who had pathologic lesions on CT SAG T2WIs, 40 patients (mean age, 69 years; range, 54-81 years) had concurrent cervical and lumbar spinal stenosis.
Patients with cervical myelopathy can present with a broad spectrum of signs and symptoms according to the location and extent of spinal cord dysfunction. The criteria for evaluation of the severity of cervical myelopathy by the Japanese Orthopaedic Association (JOA) included upper extremity motor function, lower extremity motor function, upper extremity sensory deficits, lower extremity sensory deficits, trunk sensory deficits, and bladder function (8). If the patient presents with sensory deficits, motor weakness in the lower extremities or sphincter dysfunction, his or her symptoms and signs may be mistaken due to pathologic lesions in the lower thoracic or lumbar spine. Slipman et al. (9) reported etiologies of failed back surgery syndrome and noted that 5.6% (11/197) had unknown etiology despite a complete workup of lower thoracic or lumbar spine. We can assume that cervical myelopathy might be a cause of failed back surgery syndrome, considering its symptoms. Furthermore, motor weakness, pain, or paresthesia of the lower extremities may result from a variety extraspinal lesions including peripheral nerve compression by tumors, ganglion cysts or synovial cysts, bone excrescence, abnormal muscle origin or accessory muscle, vascular disease as well as pathologic lesions in the spine (myelopathy or radiculopathy). CT SAG T2WIs included in the lumbar spine MRI may be helpful for evaluation of obscure cervical myelopathy or exclusion of cervicothoracic myelopathy from these various causes. It allows prompt workup and treatment without additional examination of the cervicothoracic spine.
In this study, idiopathic spinal cord herniation was found on CT SAG T2WIs in two patients. Idiopathic spinal cord herniation is also known as spontaneous transdural spinal cord herniation and is a rare cause of thoracic myelopathy (10-12). However, it has been reported with increasing frequency in recent years (10). Wada et al. (11) reviewed literature on 26 cases of idiopathic spinal cord herniation. Their clinical symptoms were motor weakness, muscle atrophy, or both, presenting predominantly in a unilateral lower extremity, and sensory deficits below the upper or middle thoracic level that were sometimes strong in the contralateral side of motor weakness (Brown-S'equard syndrome). MRI is sufficient for diagnosis of idiopathic spinal cord herniation in most cases. On sagittal MR images, an anterior kinking of the spinal cord is observed with an enlargement of the posterior subarachnoid space, most commonly between the levels of the T4 and T7 vertebrae (10, 12). Patients whose symptoms are mild may be treated with less invasive therapy and monitoring (10). However, early surgical reduction of the hernia is recommended in patient with slow progressive or stepwise deterioration in the neurologic status (12). Hence, CT SAG T2WIs may be useful for detecting idiopathic spinal cord herniation which is rare but may result serious sequalae if not treated timely.
Our study had some limitations. First, this was a retrospective study depending on radiologic reports. There is the likelihood of missing pathologic lesions on CT SAG T2WIs. Considering the clinical course of the patient, reviewing the initial radiologic report would be more relevant method of following the actual management performed for the pathologic lesions of these patients. Second, diagnoses of pathologic lesions on CT SAG T2Wis, such as idiopathic spinal cord herniation or CSF leak in spontaneous intracranial hypotension, were made by MR imaging and not surgically.






 XML Download
XML Download