

 PDF
PDF ePub
ePub Citation
Citation Print
Print


Abstract
Metastases from hepatocellular carcinoma (HCC) can be found in the multiple organs including adrenal gland. But adrenal metastasis of HCC without obvious hepatic lesion is very rare. We report CT and MR findings of a patient who presented with adrenal metastasis as the first clinical manifestation of HCC. Signal intensity and enhancement pattern of adrenal metastastic mass of HCC were similar to those of HCC on MRI.
Figures and Tables
Fig. 1
Initial dynamic CT finding.
a. An arterial phase image of dynamic contrast enhanced CT scan shows a nodular surface of the liver, which is suggestive of liver cirrhosis. No liver lesion is visualized.
b, c. Arterial and venous phase images of dynamic contrast enhanced CT scan shows an ovoid, well-defined heterogeneous enhancing mass (arrow) with central necrotic portion at left adrenal gland, measuring about 5.3 × 4.4 cm in size.
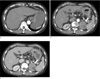
Fig. 2
Follow-up dynamic contrast enhanced CT scan obtained 4 months after the initial CT.
a, b. Arterial and venous phase images of dynamic contrast enhanced CT scan demonstratesthat the mass (black arrow, a) has increased in size. An arterial phase image reveals a tubular enhancing lesion (white arrows, a) and a venous phase image shows wash-out lesion (white arrows, b) at left portal vein, which is suggestive of tumor thrombosis.
c. An arterial phase image of dynamic contrast enhanced CT scan shows an ill-defined heterogeneous enhancing mass (arrow) at segment 4 of the liver.

Fig. 3
Gd-EOB-DTPA enhanced MR imaging findings.
a-f. Gd-EOB-DTPA-enhanced MR images show an ill-defined mass (white arrows) at segment 4 of the liver and an ovoid well-defined mass (black arrows) at left adrenal gland, with high signal intensity on T2-weighted image (a), low signal intensity on T1-weighted image (b), heterogeneous enhancement on arterial phase (c), low signal intensity on delayed phase (d), signal defect onhepatobiliary phase (e), and high signal intensity on diffusion-weighted image (f).

References
1. Katyal S, Oliver JH 3rd, Peterson MS, Ferris JV, Carr BS, Baron RL. Extrahepatic metastases of hepatocellular carcinoma. Radiology. 2000; 216:698–703.
2. Nakashima T, Okuda K, Kojiro M, et al. Pathology of hepatocellular carcinoma in Japan. 232 consecutive cases autopsied in ten years. Cancer. 1983; 51:863–877.
3. Kitagawa Y, Tajika N, Kameoka N, et al. Adrenal metastasis from hepatocellular carcinoma -- report of a case. Hepatogastroenterology. 1996; 43:1383–1386.
4. Tsalis K, Zacharakis E, Sapidis N, Lambrou I, Zacharakis E, Betsis D. Adrenal metastasis as first presentation of hepatocellular carcinoma. World J Surg Oncol. 2005; 3:50.
5. Kneuertz PJ, Demirjian A, Firoozmand A, et al. Diffuse infiltrative hepatocellular carcinoma: assessment of presentation, treatment, and outcomes. Ann Surg Oncol. 2012; 19:2897–2907.
6. Gopan T, Remer E, Hamrahian AH. Evaluating and managing adrenal incidentalomas. Cleve Clin J Med. 2006; 73:561–568.
7. Lumachi F, Borsato S, Tregnaghi A, et al. CT-scan, MRI and image-guided fna cytology of incidental adrenal masses. Eur J Surg Oncol. 2003; 29:689–692.
8. Vilanova JC, Luna A, Ros PR. Learning genitourinary and pelvic imaging. Springer;2012. p. 36–37.
9. Elsayes KM, Mukundan G, Narra VR, et al. Adrenal masses: MR imaging features with pathologic correlation. Radiographics. 2004; 24:S73–S86.
10. Johnson PT, Horton KM, Fishman EK. Adrenal mass imaging with multidetector CT: pathologic conditions, pearls, and pitfalls. Radiographics. 2009; 29:1333–1351.
 XML Download
XML Download