

 PDF
PDF ePub
ePub Citation
Citation Print
Print


INTRODUCTION
Meningiomas are common benign brain tumor which arise from the arachnoid cap or meningoepithelial cells usually located in the meningeal arachnoid area. These tumors exhibit dural attachment signs on imaging studies (1). A meningioma without dural attachment is a rare type of meningioma, and deep sylvian meningioma is one of subtype of meningiomas without dural attachment. In this study we present a case of deep sylvian meningioma.
CASE REPORT
A 43-year-old man visited our hospital emergency center with a new onset seizure. The patient had no significant past medical history. The patient had immediately undergone computed tomography (CT) and magnetic resonance imaging (MRI). The CT revealed a 15×16×16 mm rim enhancing mass located in the right deep sylvian fissure with minimal calicifications. The MRI revealed the mass as having iso-signal intensity in T1 and T2 weighted images (WI), and rim enhancement in gadolinium-enhanced T1WI with peritumoral edema. No dural tail sign was noted, which is a characteristic finding of extra-axial tumors (Fig. 1). Our first impression was a metastatic mass, with decreased certainty for brain tumors such as glioma or lymphoma.
The patient underwent a surgical resection of the tumor mass, which was found to be an extra-axial mass located in the deep sylvian fissure. There was no dural attachment.
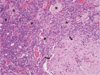
The pathologic diagnosis of mass confirmed lymphoplasmacyte-rich type meninigoma (WHO grade I) (Fig. 2). The less enhanced central portion was identified as central hyalinizing or sclerotic area, intermingling with clusters of meningothelial like cells. The immunohistochemistry profile showed positive staining of epithelial membrane antigen (EMA) and vimentin.
The patient's post-operative course was uneventful, and has returned to normal activities without any neurologic deficiencies. A follow-up gadolinum-enhanced MRI showed about 5 mm sized residual mass in the right deep sylvian fissure, which remained unchanged for 4 years after the surgery.
DISCUSSION
Meningioma is a common brain tumor which represents about 15% of primary intracranial tumors in adults. Most meningiomas present with typical dural tail sign in imaging studies, since it originates from arachnoid cap or meningothelial cells (1). A meningioma without dural attachment was first identified by Cushing and Eisenhardt (2). Furthermore, Zhang et al. (1) had classified supratentorial meningiomas without dural attachment into five types: intraventricular meningioma, pineal region meningioma, deep sylvian meningiomas, intra-parenchymal or subcortical meningiomas, and others. These investigators also classified infratentorial meningiomas without dural attachment into four types: intraventricular, inferior telachoroidea, cisterna magna, and intraparenchymal types.
Deep sylvian meningioma probably arise from the arachnoid cap cells in the arachnoid and pia of the sylvian fissure and the Virchow-Robin space of the middle cerebral artery branches (3). To the best of our knowledge, only 4 cases of deep sylvian meningioma including the present case have been reported in South Korea (Table 1). Additionally, meningiomas without dural attachment have been reported for a total of only 8 cases in Korea (7-9). In worldwide, about 28 cases of deep sylvian meningioma including our case have been reported (1-6, 10).
Meningiomas without dural attachment have been reported to mainly affect young adults with a slight male predominance (mean age of 26.5 years and 1.39 times more prevalent in males). The most common clinical presentation is seizure, and most patients are reported to have good prognosis after surgery (3). Radiologic findings are variable for this rare entity, and pre-operative correct diagnosis is difficult. On MRI, the mass is more frequently described as having iso- or low-signal intensity on both T1WI and T2WI with intense homogeneous enhancement and peritumoral edema (3). Sometimes the mass shows a calcification on noncontrast CT. However, these findings are nonspecific, and the lesion may be confused with glioma, metastasis, lymphoma, tuberculous granuloma, cavernous angioma, and craniopharyngioma.
Pathologically, the lympoplasmacyte rich type (WHO grade1) deep sylvian meningioma has never been reported.
Table. 1 summarizes the 4 reported cases in Korea, showing certain agreements with radiologic findings from previous reports.
The preoperative diagnosis of deep sylvian meningioma is very difficult. However, a deep sylvian meningioma should be considered when a well enhanced mass is observed in the fissure, even in the absence of a dural tail sign.


 XML Download
XML Download