

 PDF
PDF ePub
ePub Citation
Citation Print
Print


Introduction
Epidermoid cyst is a rare benign tumor, which accounts for 1-2% of all testicular tumors (1). It can be cured by organ preserving surgery.
We experienced a case of pathologically confirmed testicular epidermoid cyst, which showed typical onion ring appearance on ultrasonography (US) and high signal intensity with internal alternating low signal intensity patterns on T2-weighted magnetic resonance imaging (MRI). The mass revealed homogeneous high signal intensity on diffusion weighted imaging (DWI) and low apparent diffusion coefficient (ADC) value. DWI is designed to detect Brownian motion of water molecules within tissues. It is a useful imaging tool to differentiate malignancy from benign lesions (2). In the field of neuroradiology, finding of diffusion restriction has been known to be useful in diagnosing epidermoid cysts (3).
We illustrate imaging features including DWI, and ADC maps and the pathologic findings of testicular epidermoid cysts.
Case Report
An 18-year-old man presented with a nontender and palpable mass in the right testis. An elastic and firm mass without tenderness was palpable in the middle portion of the right hemiscrotum on physical examination. There was no evidence of erythema on the overlying skin or palpable lymphadenopathy. He had no history of trauma or other medical history. Sex hormones, α-fetoprotein and β-human chorionic gonadotropin on laboratory studies were within normal range.
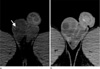
He underwent gray scale and Doppler US of the scrotum (Fig. 1). The mass showed alternating concentric rings of hypo- and hyperechogenecities with hypoechoic rim, which has been termed the 'onion ring' appearance. No vascularity was detected within the testicular mass on Doppler US study. The left testis was normal. Precontrast CT images revealed curvilinear calcification in the periphery of the testicular mass (Fig. 2A). Region of interest of the mass was measured as 25-30 HU. The testicular mass showed no enhancement on contrast-enhanced CT images (Fig. 2B). There was no evidence of significantly enlarged lymph nodes or imaging findings indicating metastasis. We considered testicular epidermoid cyst, testicular teratoma or other testicular tumors as initial diagnosis. Scrotal MRI was performed for further evaluation of the mass (Fig. 3). The mass showed low signal intensity with low signal peripheral rim on T1-weighted images. T2-weighted images revealed high signal intensity with alternating concentric and linear low signal intensity rings that was similar to the onion ring sign on the US. The mass lacked an enhancing solid portion or fat component, which is usually detected in teratomas. DWI was obtained at b-values of 50 and 800 sec/mm2. The mass showed high signal intensity on DWI with the low b-value of 50 sec/mm2 without signal drop in the high b-value of 800 sec/mm2, and lower ADC values than normal parenchyma of the testis.
Organ preserving surgery of the right testis was performed. A well-encapsulated mass of 2×2 cm in size was disclosed in the right scrotal sac and was resected. The resected mass was filled with friable and yellow-whitish materials (Fig. 4A). Upon microscopic examination, the cyst was found to be lined by squamous epithelium with a granular cell layer and fibrous wall. The mass was filled with keratinized debris and cleft space without teratomatous elements, compatible with a testicular epidermoid cyst (Fig. 4B). The surrounding seminiferous tubules showed intact spermatogenesis without atrophic change.
Discussion
Epidermoid cyst is a benign epithelial tumor that is commonly found in the brain, meninges, spleen, salivary gland, pancreas, etc. (4). Epidermoid cysts in the testis account for 1-2% of all testicular tumors (1). Epidermoid cysts can occur in multiplicity, in which case it is related to Gardner syndrome, Klinefelter syndrome, primary carcinoid tumor and cryptorchid testis. The usual clinical manifestation of testicular epidermoid cyst is a nontender, palpable and solitary intratesticular mass at 20-40 years of age. Tumor markers such as serum α-fetoprotein and β-human chorionic gonadotropin are within normal range (5).
The onion ring sign on the scrotal US was considered as a characteristic finding of a testicular epidermoid cyst (4). Although sonographic findings may suggest testicular epidermoid cyst, it is not pathognomonic because of considerable overlap with cystic teratoma (6). It has been reported that teratoma can show onion ring pattern without blood flow on color Doppler examination (7). In this case, the lesion showed an onion ring appearance on US and the US finding was pathologically associated with alternating layers of compacted keratin and loosely dispersed desquamated squamous cells (1). Teratoma of the testis has malignant potential and can cause metastasis. If teratoma of the testis is suggested, orchiectomy is needed. However, testicular epidermoid cyst is a benign lesion without recurrence, and organ preserving surgery as treatment is enough. For that reason, differential diagnosis of these lesions is important when deciding upon treatment strategy (7-9).
Calcification in testicular epidermoid cysts is occasionally noted on CT (4), as it was in our case. CT is useful in evaluating metastasis or systemic nodal staging and demonstrateing calcification. However, this finding has no more benefits for tumor characterization or differential diagnosis.
Recently, MRI has been used to differentiate epidermoid cysts from other testicular malignancies and to facilitate a precise preoperative diagnosis (10). The testicular mass in our case showed high signal intensity with internal concentric rings of alternating high and low signal intensity on T2-weighted images. The findings were concordant with the onion ring appearance on the US. Also, the peripheral low signal rim on T1 and T2 weighted images represented fibrous capsule and epithelial lining of the epidermoid cyst. The absence of contrast enhancement is associated with the benign nature of these lesions. This point helped to make a differential diagnosis from other solid testicular tumors or abscesses, which showed enhancement. Malignant testicular tumors usually show enhancing solid portions and areas of hemorrhage or necrosis. Also, a malignant testicular mass can invade adjacent organs beyond the testis. MRI can help to characterize testicular tumor due to high tissue contrast characterization. The fat component of a mature cystic teratoma appears as high signal intensity on T1 weighted images. In this case, no fat component in the mass was detected on the phase images of MRI. The testicular mass showed high signal intensity on DWI and lower ADC values than adjacent normal testicular parenchyma. The signal intensities of DWI and ADC are typical findings of epidermoid cysts in the brain. On DWI, intracranial epidermoid cysts show restricted diffusion with high signal intensity and similar ADC values to brain parenchyma. The low ADC values of intracranial epidermoid cysts were supposed to result from the dense keratinous and proteinous content, and could be applied to testicular epidermoid cysts (3). Abnormal high SI on DWI in ovarian mature cystic teratoma has been reported to correspond to keratinoid substance and Rokitansky protuberances. However, high SI in ovarian mature cystic teratoma on DWI usually presents as small focal portion of cystic mass which is different with our case that showed homogeneous diffusion restriction. Heterogeneous appearance due to stratified squamous lining, keratinoid or mucoid content, fatty component and calcified epithelial derivatives could add diagnostic value in differentiating mature cystic teratoma from epidermoid cyst. To the best of our knowledge, there have been no report about the findings of DWI and ADC map in epidermoid cysts and mature cystic teratoma of testis.
Enucleation is currently performed for testicular epidermoid cyst because it may offer better psychologic and cosmetic results, and also preserve fertility. A careful frozen section analysis and biopsies of the adjacent parenchyma can ensure this process (7). There has been no reported recurrence in patients who underwent enucleation for testicular epidermoid cysts (1). The procedure could be more safely performed if preoperative diagnosis is accurate and reliable.



 XML Download
XML Download