

 PDF
PDF ePub
ePub Citation
Citation Print
Print


INTRODUCTION
Platelet activation and aggregation are the underlying pathophysiological mechanisms associated with acute coronary syndrome (ACS) and other ischemic conditions. Clopidogrel has been recommended as an antiplatelet agent for the prevention of recurrent ischemic events. It is a prodrug that is converted to an active metabolite by the hepatic cytochrome P450 (CYP)-dependent pathway [1, 2]. The active thiol metabolite irreversibly binds to the P2Y12 ADP receptor of the platelets, which results in the inhibition of platelet aggregation [1, 2].
Many clinical studies have shown that the antiplatelet response to clopidogrel treatment has wide inter-individual variability, which may be associated with the poor clinical outcome in some patients [3-6]. Recent studies on the me-chanisms associated with clopidogrel resistance have shown that genetic polymorphisms, noncompliance, inappropriate dosage, obesity, insulin resistance, and drug-drug interactions might play an important role in the development of clopidogrel resistance [1, 2, 5, 7-9]. CYP variants involved in the metabolic activation of clopidogrel, such as CYP3A4, CYP3A5, and CYP2C19, might also play an important role in clopidogrel resistance [1, 2, 5, 8]. The CYP2C19*2 and CYP2C19*3 variants have been reported to be significantly associated with clopidogrel resistance [1, 2, 4, 8]. The aim of this study was to investigate the frequency of clopidogrel resistance in Korean patients with ACS and to evaluate the relationship between the antiplatelet effects of clopidogrel and pharmacogenetic factors. The effects of clinical and pharmacokinetic factors on clopidogrel resistance were also investigated.
MATERIALS AND METHODS
1. Patients
A total of 114 patients diagnosed with ACS at the Samsung Medical Center between June 2008 and July 2009 were evaluated. All the patients underwent coronary angiography and received a daily dose of 75 mg (105 patients) or 150 mg (9 patients) of clopidogrel for more than a month. The ages of the patients ranged from 35 to 87 yr (median age, 63 yr) and their body weights ranged from 43 to 105 kg (median weight, 69 kg). All the patients were undergoing dual antiplatelet therapy with aspirin and clopidogrel. Of the 114 patients, 32 received an additional dose of cilostazol. This study was approved by the Institutional Review Board of Samsung Medical Center, Seoul, Korea. Written informed consent was provided by all the patients.
2. Estimation of the concentration of clopidogrel
All blood samples were collected at a steady state before the next administration of clopidogrel. The plasma concentrations of clopidogrel were determined using HPLC (HPLC 1100 system; Agilent, Santa Clara, CA , USA) coupled with tandem mass spectrometry (MS/MS) (API 4000; Applied Biosystems, Foster City, CA, USA). Chromatographic separation was performed on a C18 column (2.1×50 mm, 3 µm, Atlantis dC18, Waters; Milford, MA, USA). The mobile phase consisted of deionized water and acetonitrile with 0.1% formic acid, and the flow rate was 0.25 mL/min. The mass spectrometry analysis was performed in the multiple reaction monitoring mode, where the precursor-to-product ion transition was monitored at mass-to-charge ratio (m/z) 322.1→212.1 for clopidogrel and m/z 326.1→216.1 for the internal standard (2H4-clopidogrel). The CV values for intra- and inter-day precision were less than 10%, and the calibration curve ranged from 1 to 1,000 pg/mL.
3. Evaluation of the antiplatelet effects of clopidogrel
The platelet function test was performed to monitor the antiplatelet effects of clopidogrel. The degree of platelet inhibition was determined by the VerifyNow P2Y12 assay (Accumetrics, San Diego, CA, USA). Data on ADP-induced platelet aggregation and clopidogrel-induced platelet inhibition were expressed in terms of platelet reactivity units and percent inhibition, respectively.
4. CYP2C19 genotyping
Genomic DNA was extracted from whole-blood leukocytes by using the Wizard Genomic DNA Purification Kit (Promega, Madison, WI, USA). Exon 4 and exon 5 of the CYP2C19 gene were isolated; CYP2C19*2 (681G>A; rs4244285) and CYP2C19*3 (636G>A; rs4986893) were amplified using PCR and a thermal cycler (Model 9700; Applied Biosystems). After treatment with shrimp alkaline phosphatase and exonuclease I, direct sequencing was performed using an ABI Prism 3100 Genetic Analyzer (Applied Biosystems) with a BigDye Terminator Cycle Sequencing Ready Reaction Kit (Applied Biosystems).
5. Statistical analysis
All statistical analyses were performed using MedCalc (MedCalc software; Mariakerke, Belgium). The findings for the non-responder and responder groups were compared using the Chi-square and Mann-Whitney tests. P values less than 0.05 were considered statistically significant.
RESULTS
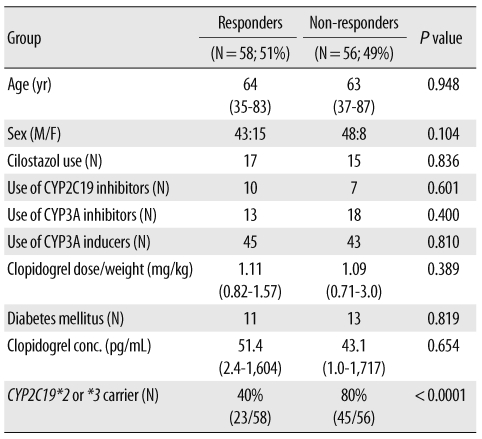
Among the 114 patients evaluated in this study, 68 (60%) were carriers for the CYP2C19*2 or CYP2C19*3 (Table 1).
There was a wide inter-individual variability in platelet inhibition (0-76%), and 56 patients (49%) showed less than 20% inhibition. Non-responders to clopidogrel treatment were more frequently found among patients with the variant CYP2C19 genes (P value<0.0001) (Table 1 and Fig. 1).
Clopidogrel concentrations ranged from 1 to 1,717 pg/mL (median, 39.5 pg/mL). There was no correlation between clopidogrel concentration and the weight-adjusted dose (data not shown). There was no difference between the clopidogrel concentrations in the responder and non-responder groups. Regarding the concentration of clopidogrel on the basis of the CYP2C19 genotype, the median concentrations of clopidogrel were 92.3 pg/mL and 34.1 pg/mL in patients with the wild-type and CYP2C19 variants, respectively (P value=0.0574).
In addition, other factors such as diabetes mellitus (DM) and concurrent medications, such as CYP2C19 inhibitors, CYP3A inhibitors, or CYP3A inducers, did not differ between the 2 study groups.
DISCUSSION
The goal of the present study was to evaluate the frequency of clopidogrel resistance and to comprehensively investigate the clinical, pharmacokinetic, and pharmacogenetic factors associated with clopidogrel resistance in Korean patients with ACS. Clopidogrel resistance was observed in 53 patients (46%) with ACS in this study. The frequency of clopidogrel resistance has been reported to range from 5% to 44% [8, 10, 11]. Clopidogrel resistance was believed to be caused by various clinical, pharmacokinetic, and pharmacogenetic factors [1, 2, 5, 7-9]. In this study, CYP2C19 genotypes were observed to have a significant association with clopidogrel resistance in Korean patients with coronary artery disease (CAD).
CYP2C19*2 is a mutation caused by the substitution of guanine with adenine at nucleotide position 681 of exon 5, which results in aberrant splicing and complete loss of CY-P2C19 activity [2, 9]. CYP2C19*3 is a mutation caused by a guanine to adenine point mutation at nucleotide position 636 of exon 4, which produces a premature stop codon [12]. Previous studies have suggested a correlation between CYP2C19*2 and clopidogrel resistance; however, most of these studies have been performed in patients from the Caucasian region, and there is very limited data on Asian populations. A previous study reported that only the CYP2C19*3 genotype was a significant risk factor for clopidogrel resistance among Korean patients with the CYP1A1, CYP2A2, CYP3A4, CYP3A5, CYP2C19, CYP2J2, and P2RY12 genotypes [8].
To investigate the pharmacokinetic factors associated with clopidogrel resistance, we quantified the plasma concentration of the prodrug clopidogrel. In procedures for quantification of active metabolites, a stabilization protocol for the unstable compounds is required [13, 14]. Although the use of special techniques for stabilizing the active metabolites was not possible in a routine clinical setting, high concentrations of the prodrug clopidogrel most likely indicated low rates of conversion of the prodrug to the active metabolite; thus, the antiplatelet effects were expected to be minimal in patients with high concentrations of clopidogrel. Patients who received clopidogrel therapy showed a wide distribution of clopidogrel concentrations. However, there was no correlation between the concentration and the weight-adjusted dose. Clopidogrel concentrations showed no correlation with other factors such as percent inhibition of platelets and CYP2C19 variants. The possible reasons for the lack of difference in clopidogrel concentrations on the basis of the CYP2C19 genotype are as follows: the potential effects of genetic polymorphisms other than CYP2C19; various clinical factors such as compliance, obesity, DM, and underlying characteristics of CAD; measurement of the prodrug clopidogrel concentration, which acted an indirect surrogate marker, rather than the active metabolite concentration; the factors associated with the sampling time for drug monitoring; and the small number of study subjects.
Pharmacodynamic response to clopidogrel was diminished by the genetic variations, but an association between the CYP2C19 genotype and clopidogrel concentrations was not observed in this study. Only 15% of clopidogrel is converted to active thiol metabolites by the CYP enzymes, while the remaining 85% is converted to inactive metabolites by esterases [5]. In addition, the levels of the prodrug clopidogrel were extremely low in comparison with the levels of the active and inactive metabolites. Other genes associated with absorption (ABCB1) and activation (CYP3A5) could also influence clopidogrel concentration. The possibility of the metabolic pathways influencing the clopidogrel response cannot be excluded. We also evaluated the possibility of drug-drug interactions leading to differences in the pharmacokinetic and pharmacodynamic characteristics of clopidogrel. Concurrent medications, such as CYP3A inducers or inhibitors, were not associated with the clopidogrel concentration or clopidogrel resistance. The clinical factors associated with clopidogrel resistance include noncompliance and insulin resistance [1]. Patients with DM have been reported to have significantly lower levels of active metabolites [1]. However, the 24 patients with DM who were on medication did not show differences in clopidogrel response in this study.
The study had the following limitations: First, only 2 allelic variants of CYP2C19 were studied. Other genes in the CYP group might also be involved in the metabolism of clopidogrel [1, 2, 7, 9]. Second, the plasma concentrations of the active thiol metabolites were not measured. Third, the number of patients was small.
In conclusion, this is the first study to evaluate the clinical, pharmacokinetic, and pharmacogenetic characteristics of clopidogrel resistance in Korean patients with ACS; the evaluations included the monitoring of clopidogrel concentrations. The results of this study confirmed that the genetic polymorphism of CYP2C19 could be important in clopidogrel response. However, further studies are required to investigate other likely factors involved in clopidogrel resistance.

 XML Download
XML Download