

 PDF
PDF ePub
ePub Citation
Citation Print
Print


INTRODUCTION
Acute promyelocytic leukemia (APL) is one of the most characteristic subtypes of AML in which abnormal promyelocytes predominate within peripheral blood or bone marrow [1]. Also, t(15;17)(q22;q21) shows a characteristic chromosomal translocation in APL, observable in 70-90% of APL patients. Owing to all trans-retinoic acid (ATRA) combined with chemotherapy, APL has one of the highest cure rates of all types of AML. Seventy to eighty percent of newly diagnosed APL patients with the PML-RARA rearrangement are cured or under long-term remission, yet some of them have a poor prognosis [2-5]. Because cytogenetics is one of the most powerful prognostic factors for the outcome of AML, cytogenetic abnormalities can cause change in treatment response, relapse, and clinicopathological characteristics [6]. Incidence of secondary cytogenetic abnormalities has been observed in ~40% of APL cases [1], but their prognostic significance is still unclear [5-7].
About 1% of the reported secondary cytogenetic abnormalities in APL patients are ider(17)(q10)t(15;17)(q22;q12), an infrequent type of additional recurrent chromosomal abnormality, according to a recent study [6]. However, ider(17)(q10)t(15;17) associated with the PML-RARA rearrangement in microgranular variant APL is even more rare. As far as we know, only 2 cases of the ider(17)(q10)t(15;17) abnormality in microgranular APL have been previously reported [8, 9]. Here, we describe an unusual microgranular APL case associated with ider(17)(q10)t(15;17), identified by both conventional cytogenetics and FISH analyses at the initial diagnosis.
CASE REPORT
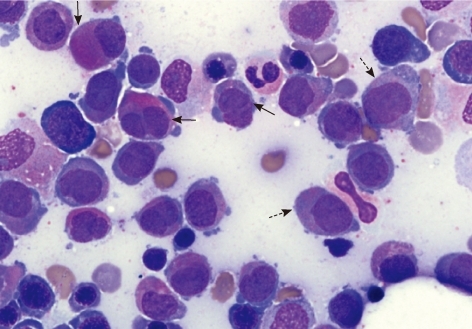
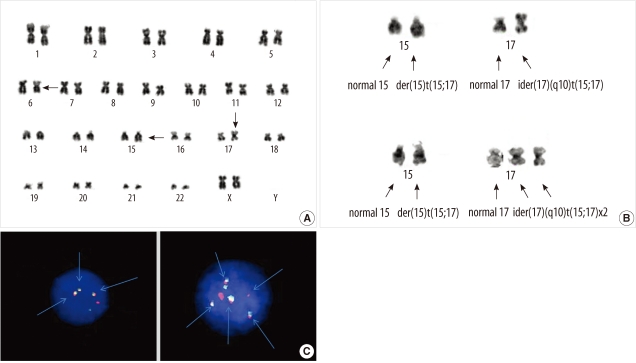
A 59-yr-old woman who had previously been diagnosed with cerebral infarction was brought to our hospital due to right side weakness in November 2007. The initial complete blood count showed pancytopenia, Hb level of 9.9 g/dL (reference range 12-16 g/dL), platelet count of 83,000/µL (reference range 150,000-350,000/µL), and white blood cell count of 1,000/µL (reference range 4,000-10,000/µL). Bone marrow aspiration showed a hypercellular marrow replaced by increased promyelocytes with a paucity or absence of granules, accounting for 36% of all nucleated cells (Fig. 1). The results of special staining of bone marrow specimens were as follows: Myeloperoxidase, positive; periodic acid Schiff, negative; Nonspecific esterase, negative. Flow cytometric analysis was conducted and showed that the blasts were positive for CD13 (91.1%), CD33 (83.9%), CD117 (59.2%), CD2 (43.9%), and CD45 (25.4%), and negative for HLA-DR (3.4%), CD3 (1.3%), CD7 (0.6%), CD10 (1.8%), CD14 (2.4%), CD19 (5.1%), CD34 (1.4%), CD41 (2.9%), CD56 (1.2%), and TdT (0.9%). Bone marrow chromosome analysis revealed a 46,XX,del(6)(?q21q25),der(15)t(15;17)(q22;q12),ider(17)(q10)t(15;17)[10]/47,sl,+ider(17)(q10)t(15;17)[3]/46,XX[16] (Fig. 2). FISH signals from PML-RARA probes (Abbott Molecular/Vysis, Des Plaines, IL, USA) yielded the results of nuc ish(PML, RARA)×4(RARA con PML×3)[24/138], (PML, RARA)×6(RARA con PML×5)[14/138], (PML, RARA)×3(RARA con PML×2)[13/138], consistent with the abnormal fusion signal patterns seen in 37% of the nuclei examined (Fig. 2). The patient was diagnosed with APL and treated with induction chemotherapy consisting of daunorubicin, cytosine arabinoside, and ATRA. After completing induction chemotherapy, follow up bone marrow examination in January 2008 showed no evidence of morphologically visible residual leukemia. The concurrent karyotype analysis result was 46,XX in all analyzed cells; and PML-RARA FISH showed "nuc ish (PML, RARA)×2 [248]" in which the abnormal signal pattern was not observed. There was no evidence of a PML-RARA fusion gene in the reverse transcriptase-PCR (RT-PCR) analysis. As indicated by follow-up bone marrow biopsies conducted until September 2008, the patient remained in complete remission. During this period, the RT-PCR analysis did not show any signs of the PML-RARA fusion gene while other cytogenetic studies also indicated normal findings.
DISCUSSION
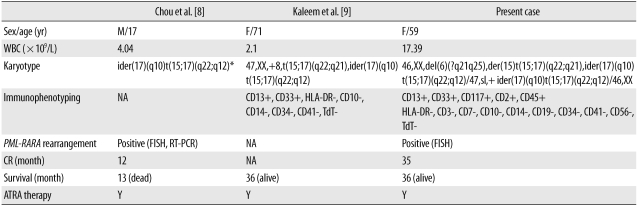
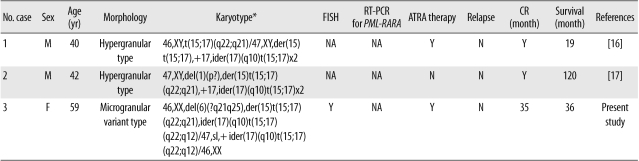
APL is a distinct subtype of AML and constitutes about 5-8% of all cases of AML diagnosis. According to the 2008 WHO classification, APL can be diagnosed when there is a t(15;17) or a PML-RARA rearrangement, even if peripheral blood or bone marrow studies show less than 20% promyelocytes [1]. As recently reported by Manola et al. [10] and our study group, the ider(17)(q10)t(15;17), an isochromosomal abnormality that occurs on the long arm of ider(17)t(15;17) after reciprocal translocation of t(15;17), is a relatively rare type of an additional recurrent cytogenetic abnormality that has been reported in 62 APL patients worldwide [8-13]. According to these studies, the influence of ider(17)(q10)t(15; 17) on the prognosis of adult APL patients is less significant than its effect on children. Indeed, 4 previously reported APL cases in children were all related to poor prognosis [8, 13-15], inferring that a more close and careful interpretation is necessary for childhood APL cases [13]. What is interesting is that so far, reports of ider(17)(q10)t(15;17) from microgranular variant (AML-M3v) type are extremely rare. Out of 62 total cases, information on APL morphology type were available in 42 cases, and most of these cases (40/42) were of the hypergranular APL type, except for 2 cases that clearly indicated AML-M3v (Table 1) [8, 9]. Therefore, further research is required to determine whether ider(17)(q10) and AML-M3v have a low association, and more careful observation should be conducted to prevent underestimating AML-M3v patients among ider(17)(q10)t(15;17) cases. Furthermore, double ider(17) (q10)t(15;17) is so rare in the International Public Databases that only 2 cases of APL patients indicating double ider(17)(q10)t(15;17) chromosomal abnormalities have been reported (Table 2) [16, 17]. In double ider(17)(q10)t(15;17), a gene dosage effect is observed owing to chromosomal abnormalities such as the PML-RARA fusion gene on chromosome 17 or the quadruplication of der(17q). In addition, since the deletion of the tumor suppressor gene TP53 occurs by the loss of 17p, further research is necessary to resolve the adverse prognosis of the APL group related to such copy number variations. Owing to the limited amount of clinical data in the literature, the relatedness between double ider(17)(q10)t(15;17) and an adverse prognosis is still unclear [16, 17]. In the case of our patient, it was hard to determine a strong association between the additional genetic aberration and prognosis because of the small clonal size of the "double ider(17)(q10)t(15;17)" abnormality.
Nevertheless, at least from a diagnostic perspective and as indicated in the authors' recent studies [13, 18], minimal residual disease detection using such multiple abnormal fusion signals through the PML-RARA FISH analysis in APL patients associated with ider(17)(q10)t(15;17) or double ider(17)(q10)t(15;17) would be considered to be a useful follow-up marker in clinical laboratories or hospitals. Additional study would contribute toward a better understanding of the influence of ider(17)(q10)t(15;17) on the prognosis, survival, and treatment response of such APL cases in adults or children. To the best of our knowledge, however, this is the third case report of microgranular variant APL associated with ider(17)(q10)t(15;17).
 XML Download
XML Download