

 PDF
PDF ePub
ePub Citation
Citation Print
Print


INTRODUCTION
The human immune system maintains the balance between protecting the host from pathologic microorganisms and avoiding excess immune reactions that could be harmful to the host [1]. Aberrant immune reactions can cause serious damage to host, such as various autoimmune and inflammatory diseases. Naturally occurring thymus-derived CD4+CD25+ regulatory T-cells (Tregs) play a critical role in the control of immune responses in various clinical settings, including autoimmune diseases, allergic disorders, infections, transplantations, and cancers [2-5].
A number of previous studies reported a high percentage of Tregs in tumor tissues and peripheral blood (PB) from patients with various cancers, including lung cancer, breast cancer, hepatocellular carcinoma, gastric, and ovarian cancer [6-9]. They showed that a high percentage of Tregs or a low ratio of CD8+ T-cells to Tregs was associated with poor prognosis and more advanced stage [7, 10, 11]. In addition to solid tumors, a few recent studies have demonstrated increased Tregs in hematologic malignancies. The increase of Tregs was stage dependent and correlated with unfavorable cytogenetics [12-14]. However, some earlier studies were limited in that they used less specific detection markers for Tregs [13, 15, 16].
In spite of the many advanced diagnostic tools, differential diagnoses between clonal or neoplastic hematologic diseases and non-clonal conditions are sometimes challenging. Since most non-clonal conditions such as aplastic anemia (AA) and primary immune thrombocytopenic purpura (ITP) are based on autoimmune processes, we can speculate that the proportion of Tregs might differ between neoplastic and autoimmune hematologic diseases. To the best of our knowledge, no previous study has directly compared Tregs between neoplastic and autoimmune hematologic diseases. In addition, most studies have shown the data for Tregs in PB, and the data on Tregs in bone marrow (BM) have been very sparse. BM Tregs have only been evaluated in neoplastic hematologic diseases.
In this study, we wanted to explore the status of Tregs and compare the proportion of Tregs between neoplastic and autoimmune hematologic diseases. Because we wanted to determine suitable conditions for Treg measurement in routine diagnostic practice, we also evaluated the technical aspects of Treg measurement, including sample types and the combination of detection markers.
MATERIALS AND METHODS
1. Study population
A total of 68 subjects were enrolled in this study from June 2009 until July 2010. There were 36 males and 32 females, and their median age was 57 yr (range, 18-85 yr). Twenty-nine subjects were diagnosed with various hematologic diseases: 11 patients with AML, 8 with MDS, 2 with AA, 5 with ITP, and 3 with autoimmune disease-related cytopenia such as systemic sclerosis or Sjogren's syndrome. The 8 patients with MDS included 1 patient with refractory anemia with ring sideroblasts (RARS), 2 with refractory cytopenia and multilineage dysplasia (RCMD), and 5 with refractory anemia and excess blasts (RAEB). The diagnoses were made by 2 hematologists following the WHO classification [17]. The patients with MDS were divided into 2 groups (low-grade and high-grade MDS) because the role of immune responses in the pathogenesis of these 2 groups is known to be different. Autoimmune processes have been suggested especially in low-grade MDS [18-20]. The low-grade MDS group included low/intermediate-1 risk, and the high-grade MDS group included intermediate-2/high risk, based on the International Prognostic Scoring System (IPSS) score. AA, ITP, and autoimmune disease-related cytopenia were categorized as the autoimmune group.
The control group (N=39) consisted of 11 patients with no evidence of specific hematologic diseases on BM examinations and 28 healthy subjects who received regular check-ups. The study groups did not differ in terms of age and sex (Table 1). This study was approved by the institutional ethics committee and informed consent was obtained from each enrolled subject.
2. Flow cytometry analysis for Tregs
PB and BM samples were obtained from all subjects, except for 28 healthy subjects in the control group, from whom only PB samples were available. The samples were collected in sterile EDTA tubes during routine diagnostic or check-up visits, and mononuclear cells (MNC) were separated by density gradient centrifugation using Ficoll (Ficoll-Paque; GE Healthcare Life Sciences, Milan, Italy). Isolated MNC layers were resuspended in phosphate buffered saline (PBS) at the concentration of 1×106 cells/mL.
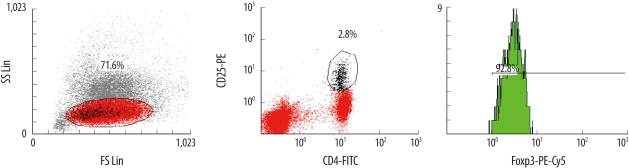
For the analysis of Tregs, a Human Regulatory T Cell Staining Kit (eBioscience, San Diego, CA, USA), including fluorescein isothiocyanate (FITC) CD4, phycoerythrin (PE) CD25, and phycoerythrin-cyanin 5 (PE-Cy5) FoxP3 (forkhead box P3) was used. Tregs were analyzed according to the manufacturer's instructions. Isotype-negative controls included a mouse isotype matched non-relevant immunoglobulin to define the positive population. After gating the lymphocyte population, the CD4+CD25high population and the CD4+CD25highFoxP3+ population were sequentially gated and analyzed. The percentage of FoxP3+ cells (CD4+CD25highFoxP3+) was counted in the CD4+ population (Fig. 1). Multicolor flow cytometry analysis was performed using Cytomics FC500 and CXP software (Beckman Coulter, Fullerton, CA, USA).
3. Statistical analysis
Chi-square test or Fisher's exact test was used for categorical variables and Student's t-test or Kruskal-Wallis test was used for continuous variables, as appropriate. Pearson's correlation was used for comparisons. The statistical analysis was performed using SPSS Software (version 14.0; SPSS Inc., Chicago, IL, USA) and MedCalc Statistical Software (version 11.2.1; Mariakerke, Belgium). P values of ≤0.05 were considered statistically significant.
RESULTS
1. PB Tregs in each group
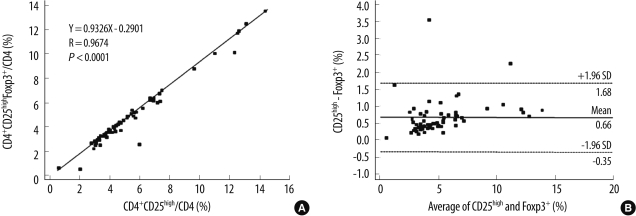
In general, the populations of CD4+CD25high/CD4 and CD4+CD25highFoxP3+/CD4 cells were significantly correlated (Y=0.9326X-0.2901, R=0.9674, P<0.0001). The CD4+CD25high/CD4 population (5.56±2.82%) was slightly larger than the CD4+CD25highFoxP3+/CD4 population (4.90±2.67%) with a mean difference of 0.66% [CD4+CD25high-CD4+CD25highFoxP3+] (Fig. 2).
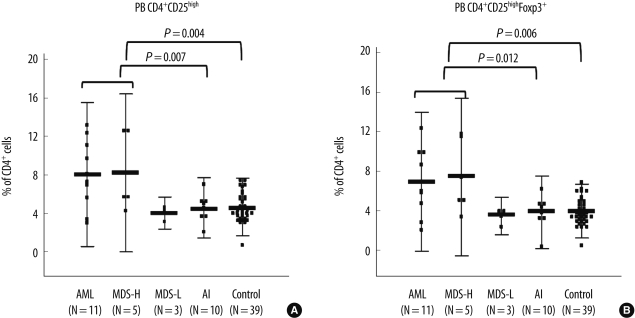
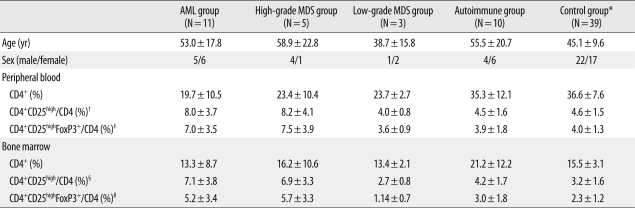
The populations of CD4+CD25high/CD4 and CD4+CD25highFoxP3+/CD4 cells in the AML group were significantly larger than those in the autoimmune (P=0.028 and 0.041, respectively) and control groups (P=0.026 and 0.035, respectively). The high-grade MDS group also had larger populations of CD4+CD25high/CD4 (8.2±4.1%) and CD4+CD25highFoxP3+/CD4 (7.5±3.9%) cells than the low-grade MDS (4.0±0.8%; 3.6±0.9%), autoimmune (4.5±1.6%; 3.9±1.8%), and control groups (4.6±1.5%; 4.0±1.3%); however, the difference was not statistically significant (Table 1, Fig. 3). When the AML and high-grade MDS groups were analyzed together as a single category, they had significantly larger populations of CD4+CD25high/CD4 and CD4+CD25highFoxP3+/CD4 cells than the autoimmune group (P=0.007 and 0.012, respectively) and the control group (P=0.004 and 0.006, respectively, Fig. 3). There were no differences in the Treg populations among the low-grade MDS, autoimmune, and control groups.
2. BM Tregs in each group
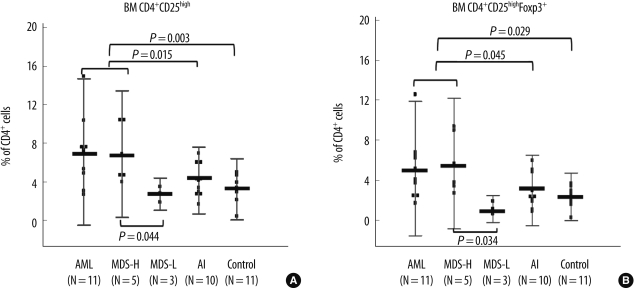
The populations of CD4+CD25high/CD4 and CD4+CD25highFoxP3+/CD4 cells were also significantly larger in the AML and high-grade MDS groups than in the autoimmune group (P=0.015 and 0.045, respectively) and the control group (P=0.003 and 0.029, respectively, Table 1, Fig. 4). In spite of the small number of patients, the high-grade MDS group had significantly larger populations of CD4+CD25high/CD4 and CD4+CD25highFoxP3+/CD4 cells than the low-grade MDS group (P=0.044 and 0.034, respectively; Table 1, Fig. 4). There were no statistically significant differences in the Treg populations among the low-grade MDS, autoimmune, and control groups.
3. Comparison of Tregs in PB and BM
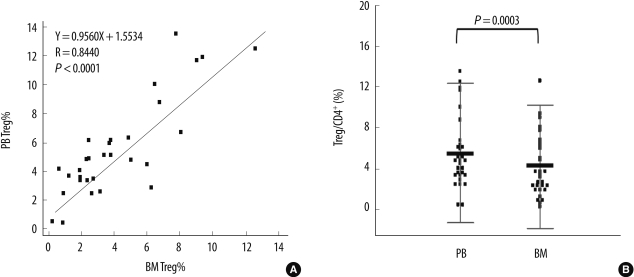
The populations of Tregs (CD4+CD25highFoxp3+/CD4) in PB and BM were significantly correlated (Y=0.9560X+ 1.5534, R=0.8440, P<0.0001). However, the Treg population was significantly larger in PB than in BM (mean difference, 1.37±1.83%; P=0.0003) (Fig. 5).
DISCUSSION
Tregs, a small subpopulation (5-10%) of CD4+ T-cells, were first described by Sakaguchi et al. [4]. Accumulating evidence shows that Tregs maintain immunologic tolerance by suppressing the activation and expansion of self-reactive immune cells, including CD4+CD25- T-cells, CD8+ T-cells, dendritic cells, natural killer cells, and B-cells, by cell-to-cell contact in a dose-dependent manner [1, 21, 22]. In addition to naturally-occurring Tregs, several subsets of Tregs, including antigen-induced Tregs (e.g., Tr1 and Th3 cells), and adaptively induced CD4+ Tregs in the periphery by conversion of CD4+CD25- T-cells and CD8+ T-cells, have been recently identified [6, 22].
In this study, we evaluated the proportion of CD4+CD25+FoxP3+ Tregs in PB and BM samples from patients with various hematologic diseases. To the best of our knowledge, no previous study has directly compared the PB and BM Treg populations among clonal and autoimmune hematologic diseases. Moreover, there has been very little data on the distribution of Tregs in normal healthy Asian populations.
According to our data, the percentage of CD4+CD25highFoxP3+ Tregs in the control group was 4.0±1.3% in PB and 2.3±1.2% in BM. Treg data in control individuals varied widely across studies, ranging from 0.5% to 12% in PB; and the percentage of Tregs in BM was consistently lower than in PB [15, 23-26]. Such wide variation may be due to differences in detection markers, gating strategies, and parameters. Although most studies analyzed the percentage of Tregs within the CD4+ cell population using CD4, CD25, and FoxP3, some studies used only CD4 and CD25 or other parameters such as absolute counts and percentages in total lymphocytes [12, 24]. In almost all these studies, the number of control subjects was very limited. Moreover, very heterogeneous groups of patients were used as controls, and most of them could not be considered as true healthy, reference individuals. Therefore, both assay standardization and determination of the reference range in each ethnic population using large numbers of healthy individuals are needed for the routine clinical use of Tregs.
In our study, the AML and high-grade MDS groups had significantly increased Treg populations in both PB and BM compared with the control and autoimmune groups. Recently, an increased proportion of Tregs in PB was reported in hematologic malignancies such as AML, multiple myeloma, chronic lymphocytic leukemia, lymphoma, and high-grade MDS [22, 25]. In clonal hematologic diseases, increased Tregs in BM was also significant, which was in agreement with previous studies [16, 18]. Although the results for Tregs in BM and PB were well correlated, the proportion of Tregs was lower in BM, and the difference in BM between groups was less significant.
Regarding autoimmune hematologic diseases such as AA and ITP, a few recent studies reported reduced proportion and function of Tregs in PB [24, 26, 27]. In addition, there is evidence for an association between early-stage MDS and autoimmune manifestations, which has not been shown for high-grade MDS [19]. A recent study reported a lower proportion of PB Tregs in early MDS [18]. In our study, the low-grade MDS group also had a low proportion of Tregs in both PB and BM, which was comparable to those of the autoimmune and control groups.
Tregs are identified by the expression of CD25, which is a component of the high affinity interleukin 2 receptor, and is functionally essential for Treg development. However, CD25 is known to be not specific for Tregs, since it is also expressed by effector T-cells. To date, expression of FoxP3, a member of the forkhead/winged-helix family of transcriptional factors, is considered an optimal marker for Tregs [1, 28]. Nevertheless, our data showed that CD4+CD25high/CD4 and CD4+CD25highFoxP3+/CD4 cell populations were significantly correlated (P<0.0001). In addition, the PB CD4+CD25high/CD4 and PB CD4+CD25highFoxP3+/CD4 populations were significantly different between the groups with neoplastic disease and the autoimmune and control groups (Fig. 3).
Regarding sample type, the Tregs in PB differed more significantly between groups than those in BM. Previous studies showed that increased Tregs in cancer is a generalized phenomenon, both in the tumor microenvironment and in PB [22]. From a technical point of view, BM processing is more difficult due to fat tissues and lower lymphocyte proportions; thus, sampling from PB would be better than sampling from BM for Treg measurement in routine clinical settings. However, the clinical significance of Tregs in PB and/or BM needs to be further evaluated using large clinical data sets.
In conclusion, this study directly compared Tregs in various hematologic diseases, including AML, MDS, and autoimmune hematologic diseases. In spite of the limited study population, our data would be useful in understanding the different immunologic bases of various hematologic diseases. Measurement of Tregs using CD4, CD25, and/or FoxP3 in PB rather than BM seems to be practical for routine hematologic purposes. The diagnostic role of Treg measurement needs to be further evaluated with a larger clinical data set.
 XML Download
XML Download