

 PDF
PDF ePub
ePub Citation
Citation Print
Print


INTRODUCTION
Bacillus Calmette-Guërin (BCG) has been traditionally used as a vaccine against tuberculosis. Further, intravesical administration of BCG has been shown to be effective in treating bladder cancer [1]. BCG contains a live attenuated strain of Mycobacterium bovis (M. bovis BCG); however, complications after bladder instillation of BCG are extreme-ly rare [2]. The few complications reported to date include high temperature followed by hematuria or granulomatous prostatitis, epididymo-orchitis, urethral obstruction, and systemic disease followed by dissemination of bacteria into other organs [3-5]. Here, we report a case of a M. bovis BCG infection that occurred after intravesical BCG therapy for bladder cancer.
CASE REPORT
A 67-yr-old male patient presented at our institution with azotemia. Three months before consulting our institute, he had visited a local clinic because he had been experiencing general weakness and poor oral intake. Biochemical and ultrasonographic examinations performed at the clinic, revealed elevated serum creatinine and obstruction of the left ureter, respectively. Other than a weight loss of 10 kg, the patient did not show any clinical features associated with M. bovis BCG infection, such as fever, chills, and night sweats. Right antegrade pyelography showed mild hydroureteronephrosis with focal stenosis in the ureteropelvic junction. The patient's history included diabetes mellitus and chronic renal failure for which he had received intermittent hemodialysis. He had been diagnosed with bladder cancer 4 yr back, and he had undergone transurethral resection of the bladder tumor (TUR-B), which was immediately followed by intravesical BCG therapy (Tice strain BCG; 12.5 mg of intravesical BCG was injected through a catheter into the bladder once every week for 6 weeks). A year later, another TUR-B was performed because atypical cells were observed in his urine, and a histological examination of his bladder indicated chronic granulomatous inflammation. Although, a diagnostic work-up for mycobacterial infections was not performed at that time, mycobacterial infection was suggested and the patient was administered isoniazid (300 mg/day), rifampicin (600 mg/day), ethambutol (800 mg/day), pyrazinamide (1 g/day), and pyridoxine (50 mg/day) for 3 months.
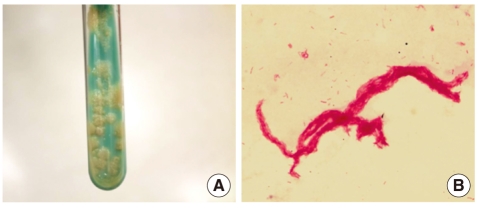
Laboratory testing performed upon admission at our institute yielded the following findings: proteinuria and pyuria in urinalysis, no microorganisms in Gram's staining of the urine sample, and acid-fast bacteria (AFB) in AFB staining of the voided urine. Mycobacteria were isolated by inoculating the patient's urine in Ogawa medium (solid egg-based medium) and by using the BACTEC MGIT 960 mycobacterial detection system (BD, Franklin Lakes, NJ, USA). The colony morphology and staining results of the isolated microorganism are shown in Fig. 1.
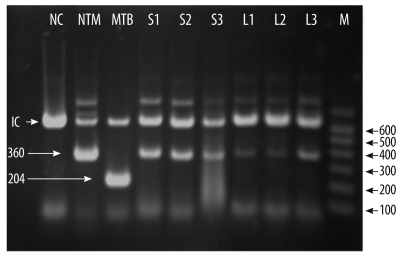
To identify the mycobacterial species present in the patient's samples, the Mycobacterium tuberculosis protein 64 (MPT-64) antigen assay, multiplex-PCR, and PCR-reverse blot hybridization assay (REBA) were performed. The MPT-64 antigen detection assay was performed using samples obtained from liquid cultures by using the TB Ag MPT64 Rapid kit (SD, Yongin, Korea). Multiplex-PCR and PCR-REBA were performed using the MTB-ID® V3 assay system (M&D, Wonju, Korea) and the REBA Myco-ID® assay system (M&D), respectively. The MPT-64 antigen is typically detected in specimens containing members of the M. tuberculosis (MTB) complex, which includes M. tuberculosis, M. bovis, Mycobacterium microti, Mycobacterium africanum, and other mycobacterial species. However, we did not detect this antigen in specimens from this patient. Multiplex-PCR allows differentiation of M. tuberculosis and mycobacterium other than tuberculosis (MOTT) on the basis of the band sizes (204 bp and 360 bp, respectively). In this study, we observed a band of 360 bp (Fig. 2). PCR-REBA allows differentiation of the MTB complex and non-tuberculous mycobacteria (NTM) on the basis of the band position on a gel strip (refer to http://www.mndkorea.co.kr for details). In this case, the band pattern obtained after PCR-REBA suggested that the isolate belongs to the MTB complex. Thus, on the basis of the results obtained after performing multiplex-PCR and PCR-REBA, the microorganism isolated from the patient's samples was suspected to be a member of the MTB complex, but not M. tuberculosis. However, the 2 PCR methods and the assay for MPT-64 antigen yielded different results.
Hence, in order to identify the causative agent we performed sequence analysis of 16S ribosomal RNA (16S rRNA) and DNA gyrase, subunit B (gyrB). For sequence analysis, DNA was isolated using the MagNa Pure LC Total Nucleic Acid Isolation Kit (Roche, Mannheim, Germany) as per the manufacturer's instructions. PCR for 16S rRNA and gyrB gene was performed in an ABI 9700 Thermal Cycler (Applied Biosystems, Foster City, CA, USA) using the appropriate primer sets suggested by the CLSI [6] and Nakajima et al. [7]. Bi-directional sequence analysis was performed using the ABI Pri-sm BigDye Terminator Cycle Sequencing Ready Reaction kit (Applied Biosystems) on an ABI Prism 3730 Genetic Analyzer (Applied Biosystems). Sequence analysis showed that the 16S rRNA (696 bp) of the isolate had 100% similarity with that of M. bovis BCG (GenBank accession no. GU142938), M. tuberculosis (GenBank accession no. GU142936), M. caprae (GenBank accession no. NR028879), M. africanum (GenBank accession no. NR-025238), M. microti (GenBank accession no. NR025234), and M. bovis (GenBank accession no. BX248338). The analysis of the gyrB gene (479 bp) revealed a 100% similarity between the sequence of the isolate and the sequence of M. bovis BCG (GenBank accession no. AM408590, AP010918) and M. bovis (GenBank accession no. BX248334).
DISCUSSION
Complications caused by M. bovis BCG administration have been rarely reported. A retrospective study by Lamm et al. [2] suggests that local adverse effects, including cystitis, fever, hematuria, and prostatitis, are the most frequent complications, whereas extravesical complications are rare. Other local adverse effects include bladder contractures, epididymo-orchitis, ureteral obstruction, and renal abscesses with or without fistula formation. Although this patient did not show any significant symptoms, the laboratory findings indicated renal dysfunction and the results of right antegrade pyelography indicated mild ureteral stenosis. Mycobacterial infections occurring after intravesical administration of BCG have been rarely reported from Korea. Most of the cases reported to date were based on the pathological findings, and to our knowledge, there are no reports of cases in which the causative species of mycobacterium has been identified. To diagnose a mycobacterial infection, Nam et al. [8] and Jeon et al. [9] examined infected tissue showing chronic granulomatous inflammation with caseous necrosis. Lee et al. [10] and Kim et al. [11] used AFB staining to determine whether an infection was mycobacterial in nature. Son et al. [12] used PCR to determine whether an infection was caused by a mycobacterium but they were unsuccessful. Recently, Kim et al. [13] reported that a molecular method using multiplex PCR for the region of difference 1 (RD1), RD8, and RD14 can be used to confirm BCG infection. We hypothesized that M. bovis BCG was the causative agent in this case and attempted to identify this organism by mycobacterial cultivation, MPT-64 antigen assay, and other molecular methods.
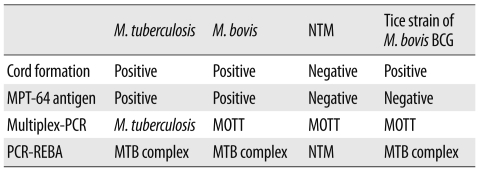
MPT-64 is a 26-kDa secretory protein produced by M. tuberculosis, and the initially purified protein was a homolog from M. bovis BCG, MPB-64 [14, 15]. The MPT-64 antigen assay can specifically detect the MPT-64 antigen secreted by the tuberculosis-causing bacteria. Usually, detection of MPT-64 antigen in this assay is suggestive of the presence of an organism of the MTB complex, which includes M. tuberculosis, M. bovis, M. microti, and M. africanum. However, some strains of M. bovis BCG, such as Copenhagen, Glaxo, Pasteur, and Tice, do not express the MPB-64 gene [16, 17]. The absence of the MPT-64 antigen in our patient can be explained by the fact that the Tice BCG strain was injected into the patient's bladder. The multiplex-PCR and PCR-REBA methods used were not helpful in confirming whether the causative agent was M. bovis because these methods could not distinguish M. bovis from other members of the MTB complexes (Table 1). The sequence analysis of 16S rRNA and gyrB gene was useful in distinguishing the members of the MTB complex, but this method had a limited ability in clearly distinguishing between the M. bovis and M. bovis BCG strains.
Although we could not confirm that M. bovis BCG was the causative agent in this case, the methods employed, which included detection of MPT-64 antigen, PCR, and sequence analysis of 16S rRNA and gyrB gene, suggest that the causative agent is the Tice strain of M. bovis BCG. This is an important finding since M. bovis BCG cannot be identified using common commercial molecular genetics tools. The patient was treated with anti-mycobacterial agents for 3 months. Subsequently, AFB staining and mycobacterial culture were performed to detect any residual mycobacterial infection, but no mycobacteria were seen in both assessments.
 XML Download
XML Download