

 PDF
PDF ePub
ePub Citation
Citation Print
Print


INTRODUCTION
Extranodal marginal zone B-cell lymphoma (ENMZL) of the mucosa-associated lymphoid tissue (MALT) accounts for 7-8% of all newly diagnosed B-cell lymphomas [1]. Usually ENMZL is an indolent disease, but some patients have shown dissemination of ENMZL into the bone marrow [2, 3].
Some studies on monoclonal gammopathy have suggested the potential of ENMZL cells to produce immunoglobulins [4-6]. The prevalence of monoclonal gammopathy in MALT lymphoma patients was reported to be 36% by Wöhrer et al. [7]. They suggested that the change in the paraprotein concentration may reflect an antitumor response. One study described that the presence of a monoclonal spike is strongly correlated with bone marrow involvement, which is indicative of advanced stages of the disease [8].
In Korea, monoclonal gammopathy in MALT lymphoma has been rarely reported until recently [9]. Here, we report a case of a 66-yr-old man diagnosed with IgM monoclonal gammopathy and ENMZL of the small intestine.
CASE REPORT
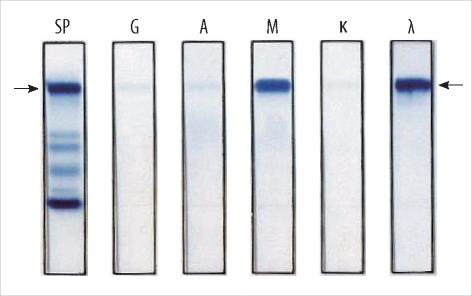
A 66-yr-old man was admitted to the hospital because of back pain and dyspnea on exertion. The patient had no history of medical illness, and he had good health until this hospital visit. Complete blood count analysis revealed that the hemoglobin level was 8.6 g/dL with microcytic and hypochromic anemia. The iron panel indicated that his anemia was caused by iron deficiency: the serum ferritin level was 5.62 ng/mL (normal range, 30-310 ng/mL) and transferrin saturation was 7.34% (20-55%). His serum chemical values were as follows: total protein, 7.9 g/dL (normal range, 6.4-8.3 g/dL); albumin, 2.7 g/dL (3.4-5.1 g/dL); lactate dehydrogenase level, 366 IU/L (240-480 IU/L); calcium level, 8.0 mg/dL (8.4-10.0 mg/dL); blood urea nitrogen, 12.7 mg/dL (6.0-20.0 mg/dL); and creatinine level, 0.8 mg/dL (0.5-1.2 mg/dL). Serum protein electrophoresis showed an abnormal zone of restriction in the gamma globin lane. The level of the M-peak was 2.1 g/dL. Serum immunofixation electrophoresis demonstrated monoclonal gammopathy of the IgM lambda type (Fig. 1).
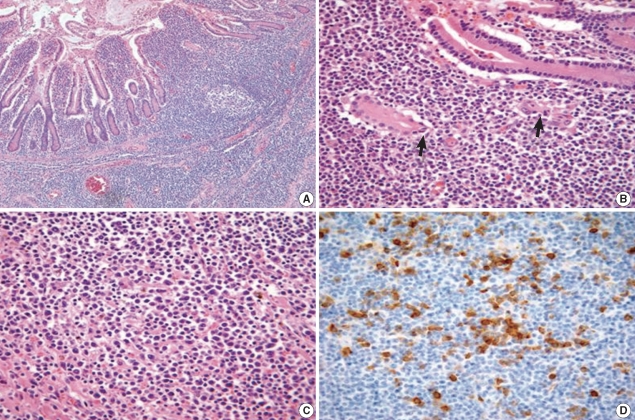
Computed tomography (CT) was performed because the patient developed abrupt severe abdominal pain. The CT scan showed a circumferential huge mass in the ileal loop along with perforation and multiple lymphadenopathy. The patient underwent an emergency operation, and he was diagnosed with ENMZL of MALT with focal large cell transformation (diffuse large B-cell lymphoma) of the small bowel. Histologic examination revealed the MZ tumor cells infiltrating around the reactive follicles and disseminating to the small bowel mucosa (Fig. 2A). The tumor cells were small to medium-sized, and they contained slightly irregular nuclei with moderately dispersed chromatin and inconspicuous nucleoli. The intestinal crypt epithelium was often invaded and destroyed by these tumor cells, leading to the formation of the lymphoepithelial lesion (Fig. 2B). Plasmacytic differentiation was observed, which was verified by immunohistochemistry for CD38 (Fig. 2C, D). Immunohistochemical analysis showed that the neoplastic lymphocytes were positive for CD20 and negative for CD5, CD10, CD23, and cyclin D1.
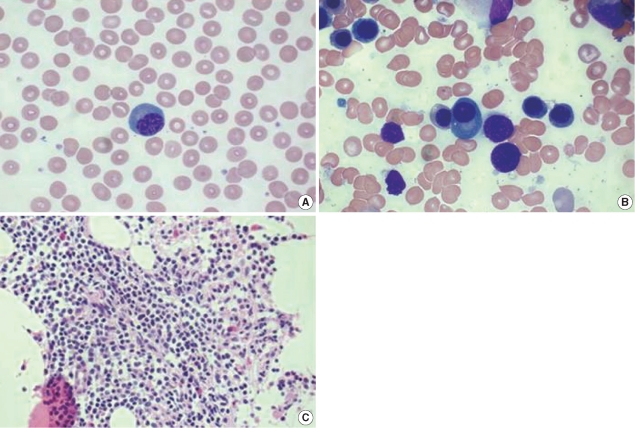
Bone marrow biopsy was performed, which showed bone marrow involvement of ENMZL. The bone marrow aspirate showed 20% cellularity and 2.1% of plasma cells (Fig. 3B). Bone marrow biopsy revealed focal infiltration of the neoplastic lymphoid cells, which showed a morphologic spectrum, including small lymphocytes with inconspicuous nucleoli and plasmacytoid lymphocytes (Fig. 3C).
A whole-body positron emission tomography (PET)-CT scan revealed a hypermetabolic mass (diameter, 7 cm) in the ileum and multiple abdominopelvic lymph node metastases. The patient was diagnosed with IgM monoclonal gammopathy and stage IV ENMZL of the small intestine involving the bone marrow and multiple abdominopelvic lymph nodes. The patient was administered a combination chemotherapy of cyclophosphamide (750 mg/m2 on day 1), adriamycin (50 mg/m2 on day 1), vincristine (1.4 mg/m2 on day 1), prednisolone (100 mg/day on days 1-5), and rituximab (375 mg/m2 on day 1) every 21 days. After the fourth cycle of chemotherapy, the patient recovered, and he is now being followed-up on an outpatient basis.
DISCUSSION
ENMZL of the MALT accounts for 7-8% of non-Hodgkin's lymphomas (NHL) [1]. ENMZL may occur in the stomach, intestine, orbit, lung, thyroid, salivary gland, skin, soft tissues, bladder, kidney, and central nervous system. The stomach is the most common site of involvement [10]. ENMZL is diagnosed on the basis of morphological examination and immunohistochemistry, including a panel of monoclonal antibodies against CD20, CD79a, CD3, CD10, CD23, CD43, Bcl-2, and cyclin D1, according to the Revised European American Lymphoma (REAL)/WHO classification [11]. ENMZL is regarded as an indolent disease, but it sometimes progresses to a more aggressive histopathogenesis and shows resistance to therapy. For patients who present with an unfavorable International Prognostic Index score and disseminated disease involving extranodal sites, the prognosis is relatively poor [2, 3].
The association of monoclonal gammopathy with B cell NHL is a well-known phenomenon, although the frequency varies between the histological subtypes. Approximately 50% of patients with lymphoplasmacytic lymphoma have elevated serum Ig levels. Paraproteinemias are often noted in patients with CLL and are less common in patients with diffuse large B-cell lymphoma [12]. The presence of monoclonal gammopathy has been reported in up to 50% of patients with splenic MZL, and it has been reported in 36% of those with ENMZL [7, 13].
Asatiani et al. [8] showed that monoclonal gammopathy in patients with ENMZL was associated with bone marrow involvement and a tendency toward large cell transformation. This study showed that the common Ig in monoclonal gammopathy was IgG, while the incidence of IgM was low (3.8%; 1/26). Our case showed bone marrow involvement and transformation from marginal zone B-cell lymphoma to large cell lymphoma in ENMZL.
The association of ENMZL with monoclonal gammopathy has been rarely reported in Korea. One case of gastric MALT lymphoma with monoclonal gammopathy but absence of Helicobacter pylori infection was reported recently in Korea [9]. Monoclonal gammopathy is negatively associated with response to eradication of H. pylori in gastric MALT lymphoma. The effect of monoclonal gammopathy on the treatment response in cases of small intestine MALT lymphoma remains unknown. The effect of changing paraprotein levels on the treatment response was observed: our patient who had a paraprotein level of 2.1-0.8 g/dL after the fourth cycle of chemotherapy showed an antitumor response. Reitter et al. [14] insisted that the paraprotein level should be routinely checked at the staging of MALT lymphoma and suggested that the change in the paraprotein level may be valuable for monitoring the treatment response.
Our report shows a rare case of monoclonal gammopathy in a patient with MALT lymphoma. Further investigations are required to determine whether the routine check for paraprotein level is needed and whether the presence of monoclonal gammopathy can assist in the prognostic stratification of patients with ENMZL.
 XML Download
XML Download