

 PDF
PDF ePub
ePub Citation
Citation Print
Print


INTRODUCTION
Therapy-related acute leukemia (t-AL) is a rare secondary leukemia that develops after chemotherapy and/or radiotherapy for primary malignancies. It can be broadly divided into 2 major groups: alkylating agent/radiotherapy-related t-AL and topoisomerase II inhibitor-related t-AL. Patients in the alkylating agent-related t-AL subgroup frequently exhibit complete or partial deletion of chromosome 5 or 7 and generally have antecedent myelodysplasia with a mean latency period of 5-7 yr [1]. In contrast, patients in the DNA topoisomerase II inhibitor-related t-AL subgroup generally develop secondary leukemia with relatively short latency periods (1-5 yr). The most common characteristic chromosomal aberrations in this group are translocations involving 11q23, i.e., the mixed lineage leukemia (MLL) gene locus [1]. Therapy-related ALL (t-ALL) is much less frequent than therapy-related AML (t-AML) and accounts for approximately 12% of all t-AL cases and 1.2-4% of adult ALL cases [2, 3].
Chromosomal 11q23 abnormalities are considered the most common karyotypic alterations with a frequency of up to 46% in t-ALL; the most common abnormality is t(4;11)(q21;q23) [2, 4].
Here, we report a case of t-ALL with t(11;19)(q23;p13.3) and the MLL-MLLT1 (alias ENL) gene rearrangement confirmed by cytogenetic analysis, multiplex reverse transcription-PCR (multiplex RT-PCR), and DNA sequencing in a patient who had undergone treatment for breast cancer. To our knowledge, this is the first report of t-ALL with the MLL-MLLT1 gene rearrangement.
Go to : 
CASE REPORT
A 40-yr-old woman underwent breast surgery for cancer of the right breast and received 6 cycles of adjuvant chemotherapy (doxorubicin 60 mg/m2 and cyclophosphamide 600 mg/m2) and radiation therapy (dose, 5,900 cGy), followed by anticancer endocrine therapy with tamoxifen. Complete blood cell counts obtained at 15 months after chemotherapy indicated acute leukemia: white blood cell count, 3.5 × 109/L with 15% blasts; Hb level, 5.8 g/dL; and platelet count, 31.0 × 109/L. Bone marrow examination showed hypercellular marrow with increased blasts, accounting for up to 95% of all bone marrow nucleated cells (Fig. 1). An immunophenotyping study using flow cytometry revealed that the blasts were positive for CD19, CD34, and cytoplasmic CD79a and negative for CD2, CD3, CD5, CD7, CD10, CD13, CD14, CD20, CD22, CD33, CD41, CD117, and myeloperoxidase. On the basis of the immunophenotype of the blasts, we diagnosed the patient with B-ALL. Cytogenetic analysis of the bone marrow aspirates by using the G-banding revealed the karyotype 47,XX,+X,t(11;19)(q23;p13.3)[4]/46,XX[16] (Fig. 2). FISH performed using LSI MLL dual color, break apart rearrangement probes (Abbott Molecular, Des Plaines, IL, USA) showed an MLL break apart signal in 76.2% of the 500 analyzed cells (Fig. 3). The MLL-MLLT1 gene rearrangement was confirmed by multiplex RT-PCR using the HemaVision kit (DNA Technology, Research Park, Aarhus, Denmark). However, 2 different amplicons (319 bp and 432 bp) were observed, and we identified the 2 amplicons by DNA sequencing. Both amplicons contained a t(11;19) (q23;p13.3)(MLL; MLLT1) translocation (Fig. 4). The patient underwent induction chemotherapy with Hyper-CVAD from March 2010. Complete remission was noted on the follow-up bone marrow study, and no MLL gene rearrangement was observed on follow-up FISH analysis. Subsequently, she underwent consolidation chemotherapy until June 2010; however, she died because of brain ischemia in the pons and the region of the middle cerebral artery.
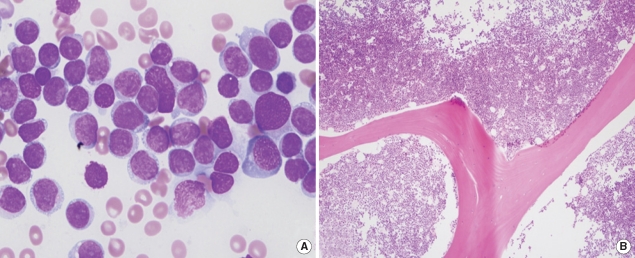 | Fig. 1Morphologic findings of B-ALL in the bone marrow. (A) Bone marrow aspirate smear shows moderate- to large-sized blasts with cytoplasmic vacuolation (Wright-Giemsa stain, ×1,000). (B) Bone marrow biopsy shows almost complete replacement of hypercellular marrow by blasts (hematoxylin and eosin stain, ×100).
|
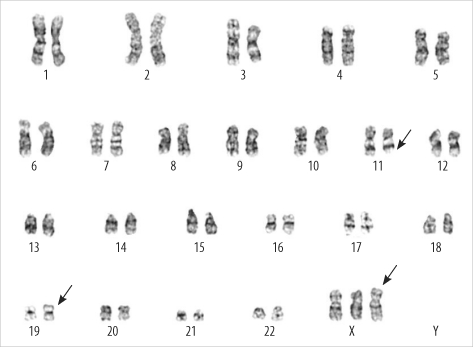 | Fig. 2G-banding of a bone marrow cell showing a 47,XX,+X,t(11;19)(q23;p13.3)[4]/46,XX[16] karyotype.
|
 | Fig. 3Interphase FISH using the LSI MLL dual color, break apart rearrangement probe (Abbott) set. Interphase nucleus harboring the MLL translocation, 1 fusion signal, and 2 separate signals (1F1O1G).
|
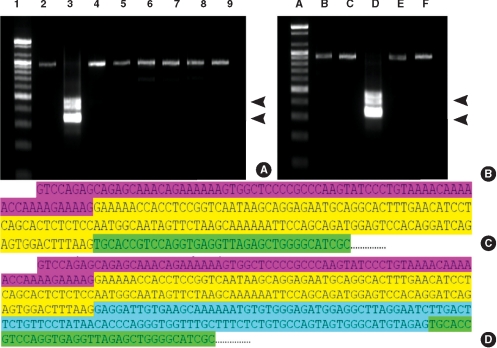 | Fig. 4
MLL1/ENL fusion transcript identified by multiplex reverse transcription-PCR. (A) Amplification products of 8 parallel multiplex reverse transcription-PCR reactions. Two bands (319 bp and 432 bp; arrow heads) are noted in lane 3. (B) Corresponding split-out reactions. Two positive bands in lane D represent the fusion transcript MLL1/ENL [t(11;19)(q23;p13.3)]. (Lanes 1 and A, 100-bp DNA ladder) (C) Part of the sequence from the 319-bp amplicon from lane D shows t(11;19) (q23;p13.3) MLL exon 9/MLLT1 exon 2. (D) Part of the sequence from the 432-bp amplicon from lane D shows t(11;19)(q23;p13.3) MLL exon 10/MLLT1 exon 2; pink, MLL exon 8; yellow, MLL exon 9; blue, MLL exon 10; green, 5' end of MLLT1 exon 2.
|
Go to :
DISCUSSION
MLL rearrangement is one of the most frequently observed genetic abnormalities in patients with t-ALL. According to a study summarizing t-ALL cases reported in the literature from 1992 to 2007, in 48 cases of t-ALL, an 11q23 abnormality involving the MLL gene locus was the predominant chromosomal aberration (32/48 [67%]), followed by t(9;22) (6/48 [13%]) and a normal karyotype (4/48 [8%]) [5]. On comparing t-ALL cases with/without 11q23 abnormalities (MLL group or non-MLL group), the distribution of primary malignancies between the 2 groups appeared to be fairly variable. Hematologic malignancies (mainly Hodgkin's lymphoma) were the most common primary neoplasms in the non-MLL group (7/16 [44%]), whereas breast cancer was the most frequent primary tumor in the MLL group (12/32 [38%]). The latency period between the primary malignancy and t-ALL in the non-MLL group was much longer than that in the MLL group (median, 36 vs. 19 months) [5]. A relatively short latency period, ranging from 12 months to 22 yr with a median latency of 16 months, has been reported in cases of t-ALL with MLL [4]. The primary malignancy in the present case was breast cancer, and the latency period was relatively short; this was compatible with the majority of previous findings for the MLL group. No significant differences were noted in the chemotherapy regimen or survival between the 2 groups.
The MLL gene on chromosome 11q23 is known to have several fusion partners. The most common partner gene is AFF1 (alias AF4) on chromosome 4q21; other common partner genes include MLLT1 (alias ENL) on chromosome 19p13 and MLLT3 (alias AF9) on chromosome 9p22 [6].
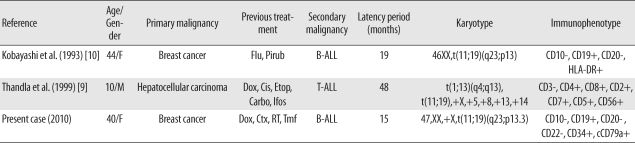
The aberration t(4;11)(q21;q23) was noted in 67-89% of MLL-positive t-ALL cases, and the aberration t(1;11)(q21;q23) was observed in 9-11% of cases [2, 4, 7, 8]. To date, only 2 cases of the aberration t(11;19)(q23;p13), i.e., involving chromosome 19p13 similar to the present case, have been reported (Table 1) [9, 10].
The breakpoint on chromosome 19 is variable [11] and can occur at either p13.1 or p13.3 [12-14]. Three MLL partner genes on 19 p13 have been identified: ELL at 19p13.1, MLLT1 at 19p13.3, and SH3GL1 (alias EEN) on 19p13.3. A report evaluating hematologic malignancy involving chromosome 11q23 and chromosome 19p13 showed marked differences between t(11;19)(q23;p13.1) and t(11;19)(q23;p13.3) [15]. Patients with t(11;19)(q23;p13.1) mostly had myeloid lineage leukemia with rare additional chromosomal changes and were predominantly adults. In contrast, patients with t(11;19)(q23;p13.3) had both myeloid and lymphoid lineage malignancy with up to 50% additional chromosomal changes and were mostly infants less than 1 yr of age. At times, the identification of the breakpoint on 19p13 by using conventional G-banding may be difficult; therefore, in the case of MLL rearrangement involving 19p13, further specific banding techniques and molecular genetic testing must be performed to identify MLL abnormalities. In this patient too, the breakpoint on G-banding was unclear; therefore, we performed multiplex RT-PCR and thereby identified the MLL-MLLT1 rearrangement. Previously reported t-ALL cases with the aberration t(11;19)(q23;p13) had not been further confirmed at the molecular level, i.e., the region of p13 on chromosome 19 that was involved was not clarified [9, 10].
Among patients with acute leukemia and MLL rearrangements, approximately 10% have been shown to have the MLL/MLLT1 rearrangement. Fu et al. [16] reported the frequency of the MLL/MLLT1 rearrangement to be 3.5% (4/114) in MLL-positive de novo AML, 23% (7/30) in MLL-positive de novo B-ALL, and 100% (4/4) in MLL-positive de novo T-ALL. Therefore, the incidence of MLL/MLLT1 rearrangement in t-ALL is significantly lower than that in de novo ALL.
The presence of the MLL/MLLT1 rearrangement appears to have certain clinical implications, such as on the prognosis. For example, non-infants with the B-ALL and the MLL/MLLT1 rearrangement have a favorable prognosis [17-21], whereas the prognosis of infants with B-ALL and the MLL/MLLT1 rearrangement is controversial [16, 17]. Further studies are essential for clarifying the clinical implications of MLL/MLLT1 rearrangement in t-ALL patients.
In a majority of t-ALL cases with the MLL rearrangement, the leukemic cells typically have a pro-B immunophenotype and are positive for CD19 and the aberrant expression of CD15 and CD65 and are negative for CD10 and CD24 patterns [6, 8, 11]. Our patient too showed a CD19-positive and CD10-negative immunophenotype; however, we did not evaluate the CD15 and CD24 immunophenotypes.
In summary, to the best of our knowledge, this is the first case of t-ALL with the aberration t(11;19)(q23;p13.3) and the MLL/MLLT1 rearrangement that was confirmed by molecular genetic testing; moreover, this case exhibited features of a CD10-negative pro-B immunophenotype similar to other cases with the MLL rearrangement.
Go to :
 XML Download
XML Download