

 PDF
PDF ePub
ePub Citation
Citation Print
Print


INTRODUCTION
Streptococcus suis is a swine pathogen that causes meningitis, septicemia, pneumonia, and endocarditis [1]. The first case of human infection with S. suis was reported in Denmark in 1968 [2], and since then, this infection has been increasingly reported in many countries [3, 4]. Until now, more than 700 cases have been reported, and most of them have occurred in Southeast Asia because of the high density of pigs in this region [3]. Three outbreaks have occurred in China, and many patients have died [1]. S. suis infection in humans has now become a great public concern worldwide. We report the case of a patient with septicemia and arthritis caused by S. suis. Cases in which S. suis is isolated from the joint fluid are very rare, and to the best of our knowledge, this is the first case report of S. suis infection in Korea. The identity of this organism was confirmed by phenotypic characterization and 16S rRNA sequence analysis.
Go to : 
CASE REPORT
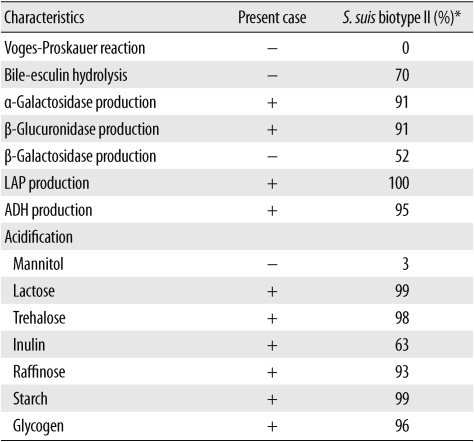
An 81-yr-old Korean woman was admitted to Konkuk University Medical Center, a secondary referral center in South Korea; the patient had arthralgia of both knees, fever, headache, and neck stiffness for 4 days before admission. Physical examination indicated tenderness and swelling in the left knee and normal lung and heart sounds. Distal motor and sensory functions were also normal. Her blood was cultured and joint fluid was aspirated; she underwent empirical antibiotic therapy with intravenous administration of cefazolin (2 g every 8 hr). Initial laboratory studies showed the following results: Hb level, 15.0 g/dL; white blood cell (WBC) count, 12.8×109/L (neutrophils, 81.1%; lymphocytes, 12.9%; and monocytes, 5.8%); platelet count, 189×109/L; and C-reactive protein level, 7.30 mg/dL. Analysis of the cerebrospinal fluid (CSF) showed no red blood cells (RBCs); WBC count, 3/µL; protein level, 50.6 mg/dL; and glucose level, 71 mg/dL. Routine biochemical tests, including liver function tests and creatinine and glucose level determination, provided normal results. Joint fluid analysis showed that the RBC count was 1,500/µL and WBC count was 76,800/µL; neutrophils were predominant among the WBCs (90%). The patient's chest radiograph showed no specific finding, and his knee joint radiograph showed severe osteoarthritis. Magnetic resonance imaging of the left knee joint showed a large amount of multiseptated joint effusion with heterogeneous signal intensity, which was suggestive of septic arthritis. The joint fluid was cultured on sheep blood agar and MacConkey agar, and blood was cultured in broth media at 37℃ (BacT/Alert; bioMérieux; Durham, NC, USA); a CSF sample could not be obtained for culture. Gram-positive cocci were cultured from the blood and joint fluid. The colonies were small, grayish, and slightly mucoid, and no hemolysis occurred on the sheep blood agar plate. The isolated infectious agent was identified by both biochemical and molecular techniques as S. suis biotype II after 24 hr of incubation. The isolate was identified on the basis of its biochemical characteristics by using the automated Vitek2 system (bioMérieux; 99.0% probability) and the API 20 Strep system (bioMérieux; 99.7% probability). The biochemical profile of the isolate is summarized in Table 1. Antimicrobial susceptibility tests were performed using Mueller-Hinton agar with 5% sheep blood; the E test was performed for penicillin and disk diffusion methods were used for other antibiotics, according to the CLSI guidelines [5]. The isolates were susceptible to penicillin (minimum inhibitory concentration [MIC], 0.047 µg/mL), cefotaxime, vancomycin, and chloramphenicol and were resistant to erythromycin and clindamycin. The identity of the isolate was also confirmed by 16S rRNA sequencing. In brief, PCR of purified DNA was performed using a thermocycler (Applied Biosystems; Foster city, CA, USA) and primers targeting the 16S rRNA region. The primer pair used for amplification was 27F (5'-AGA GTT TGA TC[A/C] TGG CTCAG-3') and 1492R (5'-G[C/T]T ACC TTG TTA CGA CTT-3') [6]. This pri-mer pair amplifies a 1,500-bp fragment of the 16S rRNA gene, which is highly conserved between different species of bacteria. The amplicons were purified, sequenced using the ABI PRISM BigDye Terminator Cycle Sequencing Kit (Applied Biosystems), and analyzed using the ABI PRISM 3730XL Analyzer (Applied Biosystems). The sequencing results indicated that the organism was S. suis strain ATCC 43765, with 99% identity. Subsequently, cefazolin was discontinued and replaced with intravenous administration of amoxicillin-clavulanate (1.2 g every 8 hr). The patient's fever subsided, and subsequent blood and joint fluid cultures were negative for streptococci and any other bacteria; however, the swelling and pain in her left knee joint persisted. She plans to undergo total knee replacement.
Go to :
DISCUSSION
S. suis is an important pathogen that causes various diseases in pigs, including meningitis, septicemia, pneumonia, endocarditis, and arthritis [4]. Human infection with S. suis has been reported in many countries, and several outbreaks have occurred in China, which has raised great public concern regarding S. suis as an emerging pathogen [1]. S. suis infection in humans has mainly been reported in countries with high population densities of pigs. A matched case-control study on the risk factors for human infection in Sichuan Province, where outbreaks have occurred, indicated that slaughtering, cutting carcasses of, and processing sick or dead pigs are the main risk factors for S. suis infection in humans [7]. Factors such as occupational or household exposure to pigs or pork may not be considered as risk factors. In some cases reported in Hong Kong and Vietnam, the patients did not report any exposure to pork [8, 9]. In the present case, the patient was from Chungcheong Province in South Korea; many pig farms were present around her house, but she was not specifically exposed to pigs or pork. Pork is the main type of meat in Korea, and housewives may come in contact with raw pork during cooking. A study has reported that S. suis was isolated from 55 of 406 palatine tonsillar samples of pigs in Korea [10]. S. suis causes a systemic infection in humans, and meningitis is the most common and serious clinical manifestation [2, 11]. Hearing loss is a frequent complication and has been reported in about half of the patients [3]. Bacteremia is also a common finding; a report on the outbreaks in China showed a high frequency of severe sepsis with high mortality rate [6]. Other clinical manifestations of S. suis infection include endocarditis, pyogenic arthritis, and peritonitis [12-15]. In the present case, the patient had arthritis and bacteremia, and joint fluid and blood culture showed the growth of S. suis. Although a CSF sample could not be obtained for culture, meningitis due to S. suis was suspected by her clinical features of severe headache and neck stiffness. However, the results of CSF analysis, such as WBC count and glucose and lactate levels, were not consistent with bacterial meningitis. A previous report on cases in Vietnam showed that S. suis is susceptible to penicillin, ceftriaxone, and vancomycin, and some strains are resistant to tetracycline (83.2% of the isolates), erythromycin (20%), and chloramphenicol (3.3%) [8].
This is the first case of human S. suis infection in Korea, and the identity of this organism was confirmed by 16S rRNA sequencing. Human infection by this organism can remain unrevealed because of incorrect identification, and infections with α-streptococci or viridans streptococci may be suggested. The majority of cases of S. suis human infection have been reported in Southeast Asia because of the high density of pigs in this region; S. suis infection may frequently occur in Korea, especially in rural areas with a high number of pig farms. Increased awareness about this emerging pathogen is needed for its detection and for prevention and treatment of diseases caused by this organism. Moreover, accurate identification of S. suis is essential, especially in cases where streptococci are isolated from the CSF, blood, or joint fluid.
Go to :
 XML Download
XML Download