

 PDF
PDF ePub
ePub Citation
Citation Print
Print


INTRODUCTION
Bacteremia or sepsis is a potentially fatal illness necessitating early diagnosis and treatment with adequate antimicrobial agents. Sepsis occurs in 750,000 people every year in the United States and has a mortality rate of 20-50% [1, 2]. Although an optimal blood culture procedure is essential for diagnosis, the positive rate is relatively low. Moreover, interpreting the results can be difficult because of the growth of normal skin flora [3, 4]. The positive rate is significantly affected by the number of blood cultures ordered as well as by the sample volume [5-9]. One set of blood cultures is not sufficient for pathogen recovery. The CLSI recommends more than 2 sets, at least 1 of which should be collected from a peripheral vessel [3, 10]
Compliance guidelines set by medical personnel is dependent on their recognition of the significance of sepsis and optimal procedures for blood culture. Large sample volumes are a burden both to medical personnel and to patients. Although the CLSI guidelines recommend a sampling volume of 20-30 mL from each venipuncture [3], this rule is often not strictly followed. The College of American Pathologists observed that the median sample volume for blood culture was 10 mL in 649 medical institutions [11]. Most hospitals in Korea do not have dedicated phlebotomists for blood culture. Therefore, quality control and continuous quality improvement, as well as education of medical personnel on proper blood culture techniques, are very important [10, 12]. While there are many reports on blood cultures based on data from individual hospitals, adequate number of multicenter studies have not been conducted. Most previous studies reported the frequency of isolates and antimicrobial resistance patterns [13-17]. Data on the number of blood cultures ordered, sample volume, and positive rate, as well as skin contamination rate, are limited in Korea, although these important parameters are necessary for blood culture quality control. We compared blood culture results from 9 hospitals while focusing on these issues and aimed to comprehensively understand the status of blood culture.
Each set of blood culture consists of an aerobic and an anaerobic bottle containing different nutrients. Recently, the usefulness of anaerobic bottles has been questioned because the incidence of anaerobic bacteremia has markedly decreased [18]. Some hospitals use a manual method for an anaerobic bottle or omit the anaerobic bottle to reduce the medical cost. However, since medically important bacteria, such as staphylococci, Enterobacteriaceae, and obligate anaerobes grow in anaerobic bottles [3, 19], it should not be omitted. We investigated the usefulness of the anaerobic bottle.
MATERIALS AND METHODS
1. Participating hospitals
All the following 9 participating hospitals are university-based: Asan Medical Center, Samsung Seoul Hospital, Seoul National University Hospital, Kangdong Sacred Heart Hospital in Seoul, Chungnam National University Hospital, Daegu Dongsan Hospital, Wonkwang University Hospital, Busan Paik Hospital, and Gyeongsang National University Hospital. The number of beds in 6 of these hospitals is 700-1,000, whereas the remaining 3 contain 1,800-2,400 beds. Most data were collected electronically.
2. Number of blood cultures ordered
The number of blood cultures ordered during January-February 2010 was examined retrospectively.
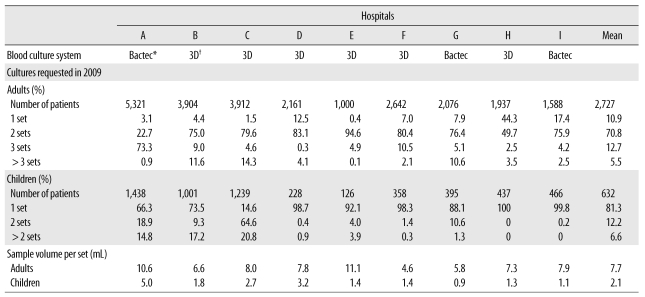
The mean number of patients in whom blood culture was performed over a 2-month period in 9 hospitals was 2,727 (SD 1,466) in adults and 632 (SD 470) in children (Table 1). The number of blood cultures ordered was analyzed in the range of 1 set to >3 sets in adults and 1 set to >2 sets in children.
3. Blood sample volume
Approximately 100 blood culture sets consisting of aerobic and anaerobic bottles were weighed at each hospital to measure the sample volume collected during a week, which was calculated by subtracting the weight of the no-sample bottles from that of the sample-inoculated bottles divided by the density of blood (1.055 g/mL) [7]. For children, 2 hospitals used pediatric bottles as well as anaerobic bottles concurrently, while the others only used pediatric bottles. Medical personnel were not informed that this study was being performed.
4. Positive rate and skin contamination rate
Rates of positive blood cultures and skin contamination were obtained using data from 2009. A positive rate was defined as the number of isolates divided by the number of requested blood cultures. Skin contamination rate was defined as the number of skin contaminants divided by the number of requested blood cultures. Skin contaminants contained coagulase-negative staphylococci (CoNS), including Staphylococcus epidermidis, Bacillus spp., Corynebacterium spp., Propionbacterium spp., Aerococcus spp., and Micrococcus spp. [3].
RESULTS
1. Number of blood cultures
Six university hospitals used the BacT/Alert 3D system (bioMerieux Inc., Durham, NC, USA) with FA and FN bottles for adults and PF bottle for children. The remaining 3 hospitals used the Bactec 9240 system (Becton Dickinson Microbiology Systems, Sparks, MD, USA) with BACTEC Plus Aerobic/F resin, BACTEC Lytic/10 Anaerobic/F, or Anaerobic/F for adults and PEDS Plus/F for children.
The rate of ordering 1 set in adults was found in less than 10% of the cases in 6 hospitals (Table 1). However, this value was 44.3% in 1 hospital. The rate of ordering 2 sets in 7 hospitals was 75.0-94.6%. The rate of ordering 3 or more sets was less than 20%, except 1 hospital (74.0%). The average percentages of adult patients in whom 1, 2, and 3 sets or more were ordered were 10.9%, 70.8%, and 18.2%, respectively.
In children, 1 set was ordered in 66.3-100% of cases in 8 hospitals, while the remaining hospital ordered 2 sets in 64. 6% of cases. The average percentages of children in whom 1, 2, and >2 sets were ordered were 81.3%, 12.2%, and 6.6%, respectively.
2. Blood volume
Sample volumes differed by each hospital. The average volume in 1 set was 7.7 mL (95% confidence interval [CI], 6.4-9.1 mL) in adults, and 2.1 mL (95% CI, 1.2-3.0 mL) in children. The range of sample volume per set was 4.6-11.1 mL in adults and 0.9-5.0 mL in children (Table 1).
3. Positive rate and skin contamination rate
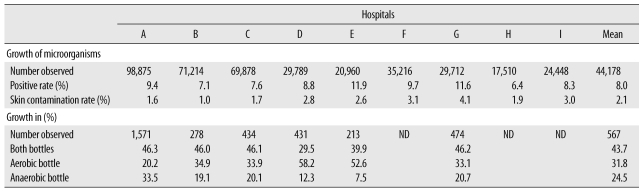
The rate of positive blood cultures in the 397,602 sets requested in 2009 was 8.0% (range, 6.4-11.9%) (Table 2). The growth rate of skin contaminants in 31,708 isolates was 26. 1%, and the skin contamination rate in the requested blood cultures was 2.1%. Of the 8,278 skin contaminants, CoNS was the most common (87.3%), followed by Bacillus spp. (5.7%), Corynebacterium spp. (3.3%), Propionibacterium spp. (1.8%), Micrococcus spp. (1.7%), and Aerococcus spp. (0.2%).
4. Comparison of isolates according to bottle
The isolation rate when using both aerobic and anaerobic bottles was 43.7%; 31.8% isolates showed growth only in the aerobic bottle, while 24.5% grew only in the anaerobic bottle (Table 2). Obligate anaerobes accounted for 11.7% of isolates, whereas CoNS (17.5%), Escherichia coli (15.6%), Staphylococcus aureus (11.6%), Enterococcus spp. (10.9%), Streptococcus spp. (6.9%), and Klebsiella pneumoniae (5.8%) were relatively common among the 833 isolates growing only in the anaerobic bottle.
DISCUSSION
Most previous reports examining blood culture techniques in Korea have used data collected from a single institution. These studies focused on changes in common pathogens and antimicrobial resistance patterns over time [13-16]. However, since laboratory facilities or personnel are nearly the same by each institution, it is difficult to evaluate whether the performance of blood culture tests is suitable. We investigated the performance of blood culture tests by comparing data from various hospitals over the same period. Because most laboratories did not use different barcodes for aerobic and anaerobic bottles from a single patient, we investigated the growth in each bottle prospectively. The numbers of blood cultures obtained from each hospital are uneven due to differences in hospital size or physician awareness of the importance of blood cultures. Multicenter participation was used to clarify the status of blood culture tests and to identify problems with the technique. All institutions were tertiary-care hospitals spread across the country. Blood was collected by interns rather than dedicated phlebotomists at all institutions.
By using only 1 set of blood culture, not only might the causative pathogen remain undetected, but it might also be difficult to interpret the results of skin contaminant [1, 3]. One institution exhibited a very high rate (44.3%) of 1set orders, revealing the urgent need to educate medical personnel. Although 3 sets of blood cultures are ideal, all but one of the laboratories generally used 2 sets. Adding a third set of blood cultures increases the sensitivity by 7.8-12.4% [20, 21]. Cockerill et al. [6] reported that the isolation of microorganisms by using the Bactec 9240 system was successful in only 65.1% of cases in which 1 culture set was used, in 80.4% of cases in which 2 culture sets were used, and in 95.7% of cases in which 3 culture sets were used. Lee et al. [8] reported slightly better results: 73.1% using 1 culture set, 89.7% using 2 culture sets, and 98.2% using 3 culture sets. Although automatic blood culture systems are widely used in laboratories, isolation of microorganisms can fail due to low concentrations of pathogens or antibiotics present in the sample [8]. Seven hospitals used only 1 bottle manufactured specifically for samples obtained from children, whereas 2 hospitals used 2 bottles for pediatric sampling. Although 2 or 3 sets of cultures are ideal for children as well, it is much more difficult to obtain sufficient sample amounts to conduct tests. Bacteremia attributable to obligate anaerobes is very rare in children; thus, the anaerobic bottle is sometimes omitted.
Blood volume collected is the primary determinant of blood culture success [3, 7, 8, 19, 20]. Compared with the positivity detected using a single 10-mL sample volume, positivity increases by 29.8-38% and 47.2-62% in detection using 20-mL and 30-mL samples, respectively [5, 6]. Although CLSI guidelines suggest collection of a 20-mL sample for 1 set in adults, the mean volume typically collected by physicians in our study was only 7.7 mL. Nevertheless, the rate of positive blood cultures was 8.0%, which is similar to those reported previously [16, 17, 20, 22]. Additional studies are necessary to identify the relationship between sample volume and rate of positive blood cultures. Compared to the bacterial concentrations detected in adults, children show higher concentrations of bacteria; thus, 1-2 mL of blood should be drawn from neonatal infants and 2-3 mL from older infants while not exceeding 1% of total blood volume [23]. The blood volume drawn from children was 2.1 mL per set. Since we did not analyze age or body weight of children, it is unclear whether this volume is sufficient to conduct the necessary blood culture tests. Measurement of blood volume in samples collected from children is neither practical nor significant compared to that in adults [1]. On the other hand, feedback regarding the blood volume in the bottle on a regular or irregular basis would be a good means of quality control. Furthermore, the positive rate or skin contamination rate can be used to determine an optimal procedure of blood culture [10].
The positive rate (8.0%) of blood cultures in our study is acceptable. Other studies in Korea showed positive rates of 4.6-9.6% [14, 16]. Studies in the United States showed a 7.5-12.4% positive rate and a 4.9% skin contamination rate [20, 22]. The isolation rate of skin contaminants was as low as 2.1%, which is acceptable. One study showed that half of isolates cultured were skin contaminants [24]. The highest isolation rate of skin contaminants obtained from a hospital was 4 times higher than the lowest isolation rate obtained from another hospital, suggesting a need for education and review of the skin disinfection procedure. In 1 clinical trial, physician education decreased the skin contamination rate from 5.7% to 1.95% [12]. Among the S. epidermidis isolates detected, approximately 10-20% might be true positives [9]. We did not review patient medical records but instead classified all S. epidermidis isolates as skin contaminants. Although Enterococcus spp. or viridans group streptococci can be isolated from the skin surface [6, 19, 25], these results were excluded in our study as per the CLSI guidelines. The skin contamination rate may vary according to the definition of skin contaminants in each study.
Since the 1980s, sepsis attributable to obligate anaerobes has decreased significantly [9, 18]. Some authors have questioned the routine usage of an anaerobic bottle based on this observation [26]. Growth only in anaerobic bottles was found in 24.5% of cases in our study, supporting the usefulness of this bottle not only for obligate anaerobes (11.7%), but also for medically important facultative anaerobes. One study showed enhanced isolation of clinically important bacteria by using 2 aerobic bottles with a selective anaerobic bottle [26]. The specific combination of bottles ideal for the isolation of clinically important microorganisms should be further investigated. Furthermore, the analysis of growth in each bottle should be extended for a longer period.
This multicenter study enabled us to evaluate the performance of blood culture tests at each hospital. Data regarding the number of blood culture sets ordered, sample volume, positive rate, as well as skin contamination rate were compared. Two sets of blood culture samples in adults and 1 set in children were commonly obtained in our study. The blood volume in 1 set was 7.7 mL in adults, which is less than that recommended by the CLSI. These data indicate that more sets should be ordered to ensure an adequate blood sample volume. Education is also necessary to decrease the skin contamination rate. Because approximately 25% of bacteria grew only in the anaerobic bottle, the anaerobic bottle should not be omitted.
 XML Download
XML Download