

 PDF
PDF ePub
ePub Citation
Citation Print
Print


INTRODUCTION
Meckel's diverticulum is considered the most prevalent congenital anomaly of the gastrointestinal tract, affecting 2% of the general population. Most Meckel's diverticula are asymptomatic and are found incidentally during laparotomy performed for other pathologies; however, the life time complication rate has been reported to be around 4%.(1)
It may give rise to bleeding (11.8%), intestinal obstruction (36.5%), inflammation (12.7%), intussusceptions (13.7%) and neoplasm (3.2%). However, perforation of Meckel's diverticulum by foreign bodies is extremely rarely seen and, in a review, was reported as being responsible for 0.5% of symptomatic diverticula.(2-4)
To our knowledge, this is the first reported case of perforation of Meckel's diverticulum by a chicken bone in Korea, and there have been few reported cases of Meckel's diverticulum perforation by a chicken bone; which were preoperatively suspected as bowel perforation.
Therefore, we report this successfully treated case of perforation of Meckel's diverticulum by a chicken bone which preoperatively presented as bowel perforation with a brief review of the relevant literature.
CASE REPORT
A 46-year-old man was admitted to emergency services with a 1-day history of lower abdominal pain that had become more severe over the previous 2 hours, accompanied by abdominal distension and loss of appetite. The patient was not receiving any specific medication and his medical history did not suggest any major disease. Physical examination revealed localized muscle guarding and abdominal tenderness below and slightly to the right of the umbilicus. Laboratory findings were as follows: WBC, 12,300/mm3; hemoglobin, 15.4 g/dl; platelet, 214,000/mm3; and C-reactive protein (CRP), 48.5 mg/dl.
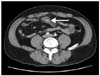
The abdominal x-ray examination showed no signs of acute abdomen. Although pneumoperitoneum was not identified, the mass-like lesion was considered to be an abdominal abscess caused by perforated bowel due to a suspicious foreign body on abdominal computed tomography (Fig. 1).
After a lower mid-line incision, some amount of serous peritoneal fluid was observed. The appendix was identified as normal. An examination revealed a perforated Meckel's diverticulum due to a foreign body approximately 100 cm proximal to the ileocecal valve (Fig. 2A). The Meckel's diverticulum was perforated by a foreign body (Fig. 2B) and the extirpated foreign body was found to be a chicken bone (Fig. 2C).
A segmental resection of the ileum, including the perforated diverticulum, was performed and bowel continuity was restored with side-to-side anastomosis by linear stapler. Additionally an appendectomy was performed. The peritoneal cavity was irrigated thoroughly with normal saline solution and Jackson-Pratt drains were placed in the right subdiaphragmatic area and in the pelvis.
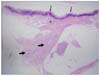
The sectioned specimen showed submucosal gastric glands and ectopic pancreatic tissue in the diverticulum wall and the mesenteric nodular mass was well developed pancreatic tissue (Fig. 3).
The patient recovered uneventfully and was discharged on the 8th postoperative day. At the follow-up examination 3 months after surgery, he was doing well.
DISCUSSION
Anatomically, the Meckel's diverticulum is a true diverticulum containing all layers of the small intestine, arising from the anti-mesenteric border of the ileum and receiving its blood supply from a remnant of the vitelline artery, which emanates from the superior mesenteric artery. Up to 60% of Meckel's diverticula harbor heterotopic mucosa, of which more than 60% contain gastric mucosa. Other heterotopic tissues include pancreatic acini, Brunner's glands, pancreatic islets, colonic mucosa, endometriosis, and hepatobiliary tissue.(5,6) Our case of Meckel's diverticulum developed at approximately 100 cm proximal to the ileocecal valve and had submucosal gastric glands and ectopic pancreatic tissue in its wall.
As a congenital variant, Meckel's diverticula are often found in children and most adults patients are asymptomatic; it has been estimated that more than 50% of those who develop symptoms are less than 10 years of age. In adult patients, intestinal obstruction is the most common complication with incidence rates varying from 22% to 50%. The most common causes of obstruction are intussusception or invagination, with the Meckel's diverticulum as the lead point. Other causes of obstruction include volvulus around fibrous bands adherent to the umbilicus, inflammatory adhesions, Littre's hernias and diverticular strictures. The second most common complication in adults appears to be related to an inflammatory process. Meckel's diverticulitis, clinically undistinguishable from acute appendicitis, occurs in about 20% of patients. It results in distal inflammation, necrosis, or even perforation, leading to abscess or peritonitis. Hemorrhage is a more common presentation in children and is reported in over 50% of cases in children. In adults, hemorrhage occurs often but is the presenting complaint in only 11.8%.(3) Perforation of MD by foreign bodies is extremely rare and in a review, the indication rate for a resection due to perforation by foreign body was reported to be 8% of all complicated diverticula.(7) There are several case reports in the literature regarding perforations caused by toothpicks, fishbones, Button battery, chicken bone, and needles.(7-9) There seems to be a tendency for foreign bodies to lodge in the blind pouch of Meckel's diverticulum. In our case, the patient presented with symptoms of acute abdomen, with preoperative CT scanning revealing bowel perforation, confirmed at laparotomy as Meckel's diverticulum perforation by a chicken bone that had been swallowed unintentionally.
It is difficult to make a preoperative diagnosis of Meckel's diverticulum. CT scan and sonography are usually of little value as distinction between a diverticulum and intestinal loops is difficult. Therefore, in all previously cases reported in the literature, the diagnosis of foreign body perforation of Meckel's diverticulum was only made when patients underwent surgery for suspected acute appendicitis.(10) However, in our case of perforated Meckel's diverticulum, although preoperative CT findings suggested bowel perforation by a foreign body such as an animal bone, we were unable to tell that the perforated site was a Meckel's diverticulum. This suggests that careful examination of a preoperative CT scan can indicate the possibility of perforation of Meckel's diverticulum by foreign body.
We therefore report this rare case in the hope that it may remind the physician of this interesting anomaly when evaluating the acute abdomen by preoperative CT scan.

 XML Download
XML Download