

 PDF
PDF ePub
ePub Citation
Citation Print
Print


INTRODUCTION
Around 6th weeks of gestational age, the midgut herniates through a defect of the umbilical cord and returns to the abdominal cavity by the 10th to 12th week of normal development. It undergoes elongation and rotation along with closure of the umbilical ring to complete that of postnatal life. Umbilical cord hernia is a simple failure of the midgut to return to the peritoneal cavity at 10~12 weeks and contains only small bowel and much smaller in defect (<4 cm) than omphalocele with relatively low incidence of associated anomalies.(1) Surgeons can easily close the defect at the initial operation with reconstruction normal appearing umbilicus. Religation of the umbilical cord after reduction of content should be avoided because any part of the bowel could be adherent to the sac.(2)
We present a neonate with umbilical cord hernia who underwent appendectomy for a successful closure of defect with umbilicoplasty.
CASE REPORT
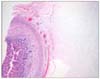
A 3,470-g baby boy was delivered vaginally at 36+1 weeks' gestation to a 27-year-old healthy mother and was immediately transferred to our ER because baby had a small omphalocele contained bowel loops in mid abdomen. On physical examination, other external appearance was normal and baby was active and good in general condition. The occlusive dressing was applied for sac protection. Preoperative laboratory findings and radiologic studies (chest x-ray and abdominal ultrasonogram) were unremarkable. Echocardiography showed small ASD and PDA. Under the general anesthesia, we firstly attempted to reduce the contents with the sac intact but failed. Upon opening the sac, small portion of terminal ileum, appendix, cecum, and ascending colon were seen. Serosa of the herniated bowel and inner surface of the sac were congested. Appendix was coated with thin hyperemic fibrinous membrane and tip of the appendix was adherent to the inner surface of the sac. Thin fibrotic band was attached to the sac and the cecum (Fig. 1). Usual inversion appendectomy and lysis of band were performed. The sac was excised along the skin edge by individual ligation of the umbilical vessels and urachus. After reduction of the abdominal contents, fascial closure and umbilicoplasty were done. Histologic examination of the excised specimen revealed a fibrinoid band between the sac and appendix with congested small vessels around the appendix. There was no evidence of inflammatory infiltrates at the appendiceal wall except a few neutrophils and lymphocytes around the congested vessels and fibrinoid band (H&E stain, ×40) (Fig. 2). Postoperative course was uneventful and discharged.
DISCUSSION
Umbilical cord hernia is a small defect of midline abdominal wall containing with herniated small bowel only in the sac. It occurs in 20% of congenital abdominal wall defects.(1) The sac covers by a membrane consisting of peritoneum on the inner surface, amnion on the outer surface, and Wharton's jelly between the layers.(3) The small bowel reduction and primary closure of facial and skin defect can nearly always be closed at the initial operation. Usually enough skin is available to reconstruct a normal appearing umbilicus. Any part of the bowel could be adherent to the sac and reduction in the sac intact is impossible. In that case, surgeons must open the sac, confirm the herniated viscera, and close the abdominal wall defect after excision of the sac. In the presenting our case, distal portion of the vermiform appendix is adherent to the inner layer of the sac and cecal wall was connected with the sac by thin fibrous band. When the appendix alone failed to re-enter the abdomen and protruded in the umbilical cord, primary nomenclature of this anomaly is "umbilical appendix".(4) Fuijkschot et al.(4) collected a total 9 cases of umbilical appendix including their own case (1 case) by searching literature dating from 1922 to 2006. Neonatal umbilical appendices cause undried umbilical cord with delayed separation, and persistent umbilical stump or persistent umbilical discharge after cord separation and are misdiagnosed to have umbilical polyp, omphalomesenteric duct remnant, or urachal remnant.(4-8) And also medical procedures like umbilical cannulation and clamping of the umbilicus may produce an iatrogenic appendico-umbilical fistula unless special attention is paid (4-8).
Borgna-Pignatti et al.(6) hypothesized that the delayed separation of an appendix-containing umbilical stump represents the possibility of the small omphalocele. Authors suggest that 'umbilical appendix' may be an overlooked umbilical cord hernia containing appendix only.
Umbilical cord hernia is considered easy to be repaired and has an excellent prognosis. Nevertheless, some tiny contents such as appendix might be damaged without careful attention. Molenaar and Tibboel(2) have described re-ligation of the umbilical cord after reduction of omphalocele content should be avoided because an open omphalomesenteric duct or some other part of the bowel might be included in the ligature.
We advocate exploration of sac content whenever some doubt in complete reduction of the content into the abdominal cavity through umbilical ring, even if the sac is very small and herniated contents reduce easily by squeezing or twisting of the sac, which could prevent appendiceal injury and future fistula as well.

 XML Download
XML Download