

 PDF
PDF ePub
ePub Citation
Citation Print
Print


INTRODUCTION
Transverse myelitis (TM) is a focal inflammatory disorder of the spinal cord. Carbamazepine is widely used to relieve the neuropathic pain, but it is frequently associated with neurologic adverse events, Stevens-Johnson syndrome (SJS), and hepatic side effects. Carbamazepine-induced liver injury is less common, but the consequences of the side effects can be very serious, leading to death or a need for liver transplantation. We report a case of a 60-year-old female with fulminant hepatic failure (FHF) and SJS induced by carbamazepine who successfully underwent deceased donor liver transplantation (DDLT). This is the first report in which neurologic and graft function in a patient with TM, FHF, and SJS recovered completely after DDLT.
CASE REPORT
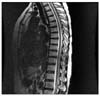
The patient, a 60-year-old female, was admitted to a neurologic department in another hospital for sensorimotor weakness of lower extremities. T2-weighted magnetic resonance imaging of the spine revealed diffuse and ill-defined high signal intensities at the T8-10 level compatible with the neurologic deficit (Fig. 1). With the results of other laboratory tests, she was diagnosed as idiopathic TM and was treated with intravenous high-dose steroid. After the pulse therapy, the motor power of the lower extremities had improved significantly but she complained of intermittent lancinating pain in the legs. The patient had been treated with carbamazepine (200 mg twice daily) in another hospital to control her sensory symptom. Fifty days after starting carbamazepine, she developed jaundice, erythematous papules, bullae, and skin erosions (Fig. 2). The patient was transferred to our liver unit because of acute liver insufficiency and a slowing of mentation, which was attributable to the carbamazepine.
On the initial physical examination, she was somnolent, but arousable. She was jaundiced and covered with erythematous macules and papules. The carbamazepine was stopped immediately. The neurologic examination revealed a motor weakness in both lower legs, graded as 1/5 according to the Medical Research Council grading system for muscle strength below the knee. A dermatologic consultation was obtained, and the diagnosis of SJS was considered. She went into severe hepatic coma in association with elevation in the serum transaminase levels and a decrease in the prothrombin index. The maximum bilirubin concentration in the blood was 22.5 mg/dl and the peak AST, ALT, and ALP were recorded to be 583 U/L, 738 U/L, and 615 U/L, respectively. Her coagulation profile became abnormal, with an INR of 6.26 (normal range, 0.9~1.2). The blood ammonia level was elevated to 393µg/dl (normal range, 19~87µg/dl). The serologic tests for hepatitis were negative. The level of consciousness decreased progressively and she became comatose. She was transferred to the intensive care unit and placed on mechanical ventilation. On the initial abdominal computed tomography (CT), a large amount of ascites and splenomegaly were noted. On brain CT, cerebral edema was not noted. She was placed on the national emergency liver transplant waiting list. Her condition deteriorated rapidly and the model for end stage liver disease score was 39. Despite continuous renal replacement therapy, she did not recover, but deteriorated and developed pulmonary edema. Fortunately, 5 days after listing, a suitable deceased donor became available, and she underwent DDLT. The pathologic findings of the explanted liver showed massive hepatic necrosis (Fig. 3). Immunosuppression was based on induction therapy with steroids and FK 506. On post-operative day (POD) 5, the SJS gradually improved. Seven days after DDLT, she was able to open her eyes spontaneously. She was extubated 11 days after liver transplantation with full awakening and ability to expectorate. Her neurologic examination showed a quadriplegia in the immediate post-operative state, but she improved and gradually recovered the power of her extremities; by post-operative day 120 she was able to walk with a walking stick. On post-operative day 45, a fungal pneumonia occurred, but was controlled by aggressive physiotherapy and an antifungal agent. The patient underwent prolonged hospitalization for rehabilitation due to acute TM and post-operative disuse syndrome. The patient was discharged with normal graft functions 5 months after DDLT. At the 12 month follow-up, the patient had no significant pathology and was ambulating independently.
DISCUSSION
TM is a rare neurologic syndrome caused by inflammation of the spinal cord, resulting in motor, sensory, and autonomic dysfunction.(1,2) TM is an interruption of spinal cord function not caused by macrotrauma.(3) The initial symptoms usually include lower back pain, abnormal sensations, such as burning, tickling, pricking, or tingling in the legs, and paraparesis of the legs. The paraparesis often progresses to paraplegia. The pain may consist of sharp, shooting sensations that radiate down the legs. There is currently no treatment that has been clearly shown to improve the outcome in patients with TM. Treatment generally consists of supportive measures. The use of steroids to hasten recovery remains controversial, but is widely offered to patients during the acute phase.(4-6) Intravenous immunoglobulin (IVIG) is frequently used. Plasma exchange was recently shown to be effective in patients with severe, isolated CNS demyelination.(7) In the case herein, we used plasma exchange, IVIG, and high-dose steroids, which may be helpful in course of acute TM.
Muscle pain that results from TM might be treated with analgesics (such as acetaminophen), non-steroidal anti-inflammatoy drugs (such as naproxen or ibuprofen), anti-depressants, and anticonvulsant drugs (such as carbamzepine). Carbamazepine has been found to be effective in the treatment of neuropathic pain by inhibiting conduction of impulses in neurons mediating pain. In this case, the patient had neuropathic pain and paralysis, and had been treated with carbamazepine to control her pain. Of note, carbamazepine may give rise to drowsiness, dizziness, and diplopia; these effects are reversible when the dose is lowered. Carbamazepine can cause more dangerous effects, such as severe rashes, bone marrow impairment, and liver damage, ranging from an asymptomatic rise in liver function tests, to acute liver failure. These effects are uncommon, but when they occur, the drug must be discontinued. The mechanism of liver injury in carbamazepine-induced hepatitis remains poorly understood, although it is presumed to be an idiosyncratic hypersensitivity, possibly derived from a genetically-determined inability to inactivate toxic metabolites.
Carbamazepine is associated with severe skin reactions, such as SJS and toxic epidermal necrolysis (TEN).(8,9) SJS is a rare, but life-threatening skin and mucocutaneous disorder that is usually drug-induced.(10,11) Nearly one-half of cases are caused by a reaction to drugs or appear during viral infections and malignancies. Currently, there is no optimal treatment strategy for SJS. Recently, IVIG has been suggested. High-dose steroids and IVIG have been demonstrated to be of benefit in the recovery from SJS.(12) Plasma exchange is also beneficial for the treatment of SJS.
The outcomes of TM are diverse and most outcomes are associated with sequelae. There is a report that high-dose corticosteroids are effective in terms of the clinical outcome.(13) TM or SJS may be caused by a variety of immunologic mechanisms. Although we cannot prove the contribution, we believe that liver transplantation, especially with high-dose steroids, IVIG, and immunosuppressants, may be an efficacious strategy for clinical recovery from TM and SJS.
No other liver transplant patient with TM has been reported in the literature. In this case, we highlight the significant neurologic recovery from FHF and SJS induced by carbamzepine in a patient with TM and paraplegia
In conclusion, liver transplantation can be a feasible therapy for patients with carbamazepine-induced hepatic failure associated with SJS and acute TM with paraplegia.


 XML Download
XML Download