

 PDF
PDF Citation
Citation Print
Print


Abstract
Adult intussusception is rare involving of only 1% of the causes of bowel obstruction. We report a case of a 39-year-old female with intussusceptions due to inverted Meckel's diverticulum. She visited our hospital for diffuse abdominal pain during 1 week and aggravated abdominal pain for 2 days. Vital signs were stable, and there was periumbilical tenderness. She had no history of abdominal operation. CT scan showed a 3.7×2.1 cm of fatty mass with focal intussusception in the distal ileum. When the emergency operation was performed, the patient was found to be suffering from ileocolic intussusception. A manual reduction of intussusception showed inverted Meckel's deverticulum at 65 cm proximal to the ileocecal valve, and the segmental resection of small bowel including a Meckel's diverticulum was performed. Pathologic examination revealed a Meckel's diverticulum containing a 0.6×0.6 cm sized aberrant pancreas.
Figures and Tables
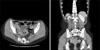
Fig. 2
Operative findings. (A) An ileoileal intussusception is noted. (B) After manual reduction of the intussusception, Meckel's diverticulum is found with a yellow colored soft mass on the tip.

Fig. 3
Histologic findings. (A) The mucosal layer is composed of gastric, colonic or small intestinal mucosa. And the proper muscle layer is also found (H&E stain, ×40). (B) In the subserosal area, pancreatic tissue is noted forming round aggregate approximately 1.0×1.0 cm in size. The pancreatic tissue is composed of ductal epithelium and scattered clusters of endocrine cells in the fibrotic background (H&E stain, ×100).

References
1. Azar T, Berger DL. Adult intussusception. Ann Surg. 1997. 226:134–138.
2. Stubenbord WT, Thorbjarnarson B. Intussusception in adults. Ann Surg. 1970. 172:306–310.
3. Brayton D, Norris WJ. Intussusception in adults. Am J Surg. 1954. 88:32–43.
4. Ymaguchi M, Takeuchi S, Awazu S. Meckel's diverticulum. Investigation of 600 patients in Japanese literature. Am J Surg. 1978. 136:247–249.
5. Schwartz MJ, Lewis JH. Meckel's diverticulum: pitfalls in scintigraphic detection in the adult. Am J Gastroenterol. 1984. 79:611–618.
6. Mackey WC, Dineen P. A fifty year experience with Meckel's diverticulum. Surg Gynecol Obstet. 1983. 156:56–64.
7. Park JJ, Wolff BG, Tollefson MK, Walsh EE, Larson DR. Meckel diverticulum: the Mayo Clinic experience with 1476 patients (1950-2002). Ann Surg. 2005. 241:529–533.
8. Pantongrag-Brown L, Levine MS, Elsayed AM, Buetow PC, Agrons GA, Buck JL. Inverted Meckel diverticulum: clinical, radiologic, and pathologic findings. Radiology. 1996. 199:693–696.
9. Daneman A, Myers M, Shuckett B, Alton DJ. Sonographic appearances of inverted Meckel diverticulum with intussusception. Pediatr Radiol. 1997. 27:295–298.
10. Hamada T, Ishida O, Yasutomi M. Inverted Meckel diverticulum with intussusception: demonstration by CT. J Comput Assist Tomogr. 1996. 20:287–289.
 XML Download
XML Download