

 PDF
PDF ePub
ePub Citation
Citation Print
Print


INTRODUCTION
Heterotaxia or situs ambiguous implies a visceral malposition and dysmorphism associated with an indeterminate atrial arrangement.(1) It can be distinguished from situs solitus (all the organs are in the normal position) and situs inversus (these organs are reversed). Generally, heterotaxia can be divided into 2 groups: asplenia (right isomerism) and polysplenia (left isomerism).(2) Polysplenia is complex and uncommon. Heterotaxia is frequently associated with a variety of gastrointestinal abnormalities, including abnormalities of intestinal rotation, asplenia or polysplenia, and biliary tract anomalies.
Intraluminal duodenal diverticulum (IDD) is also a rare congenital anomaly. It was first described by Boyd(3) in 1845, and Kinzer(4) coined the term IDD in 1949. It is regarded as a type of duodenal atresia and a failed recanalization of the duodenum.(5) IDD is frequently associated with various anomalies, and it is usually diagnosed early in life in the cases with severe obstruction. Yet most patients are diagnosed later in life because of various symptoms. Only 1 case of heterotaxia with IDD has been reported.(6) We report here on a patient with combined IDD and heterotaxia and she was successfully diagnosed and treated.
CASE REPORT
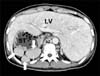
A 21-year-old female was admitted with epigastric soreness, dyspepsia and vomiting. She had been treated for gastritis and duodenal ulcer 3 years previously and she had voluntarily stopped treatment. She constantly had the symptom of dyspepsia, but she had not received medical treatment for this. She was 166 cm in height and weighed 55 kg. She was healthy without any evidence of malnutrition. All the blood tests and the chest X-ray were within the normal limits. She was referred to Department of Gastroenterology for endoscopy. A right-sided stomach and gastritis were noted on this examination, but the duodenum was not fully evaluated for the cause of the food stasis. We assumed she had situs inversus and requested a duodenography exam and computed tomography (CT). The duodenography showed the "wind sock sign" (Fig. 1) and the CT images showed a midline liver, a right-sided stomach, polysplenia, interruption of the IVC with azygous and hemiazygous continuation, and intestinal nonrotation (Fig. 2, 3). We finally diagnosed her as having duodenal obstruction due to IDD and heterotaxia syndrome. Three-dimensional virtual endoscopy by reformation of the CT angiography was carried out for evaluation of the anatomy and the severity of the IDD before treatment (Fig. 4). Endoscopic incision was attempted, but this failed, so she underwent surgery. A laparotomy was performed under general anesthesia. At laparotomy, the operative findings were the same as those of the preoperative evaluation. We performed side to side duodenojejunostomy using a GIA stapler just above the IDD. She started oral feeding 4 days after surgery and was discharged on the 7th postoperative day without complications or feeding difficulties.
DISCUSSION
Heterotaxia is a group of situs anomalies, but its nomenclature, definition and classification have been controversial. Heterotaxia was commonly confused with heterotaxy, situs ambiguous and isomerism. The International Nomenclature Committee for Pediatric and Congenital Heart Disease offered a definition of heterotaxy, but their definition is controversial because they defined heterotaxy from the viewpoint of the cardiac structures.(7)
The process and mechanism of situs anomalies has not been clearly determined. Familial situs anomalies such as Katagener's syndrome are related to autosomal recessive inheritance, but most of these patients sporadically develop their anomalies.(8) In our present case, the patient had no familial history of situs anomalies. So this case is thought to be a sporadic event. Environmental factors, including maternal DM, have been implicated in heterotaxia, but this is still not clear.(8) The true incidence of heterotaxy cannot be precisely estimated, but it occurs in approximately 1 per 10,000 people.(8) Further, this number may be higher when including the undiagnosed patients who are without serious anomalies.(8)
Most patients with heterotaxy are diagnosed early in life because of various cardiac, central nervous system, gastrointestinal and hepatic anomalies, but the patients without clinically morbid abnormalities are diagnosed incidentally.(2) Peoples et al.(9) reported that only 25% of the patients with polysplenia are alive because of the associated severe malformation. As the survival rate has become higher after heart surgery, the diagnosis and treatment of intraabdominal malformation have become important for these patients. Our patient has no cardiac abnormalities and she could be diagnosed owing to the symptoms of duodenal obstruction.
The gastrointestinal abnormalities associated with situs anomalies include various positions of the stomach and liver, malrotation, biliary atresia, multiple spleens or aspleen, and a short pancreas. Three cases of situs anomalies with IDD have been reported as a result of a search through PubMed, and only 1 case of polysplenia with IDD has been previously reported.(6)
IDD is a rare disease entity that causes duodenal obstruction. A diverticular sac is formed by the intraluminal pressure to the mucosa and submucosal membrane attached to the duodenum. Patients with IDD can have many symptoms such as epigastric pain, gastrointestinal bleeding, outlet obstruction and recurrent pancreatitis, and the typical sign seen on duodenography is called the "wind sock sign".(10) Thus, we could diagnose our patient as having IDD. Because of the advances in endoscopic techniques and instruments, endoscopic treatments instead of conservative therapy and open duodenotomy have been reported. We also attempted endoscopic incision, but we failed because of food stasis.
Three-dimensional virtual endoscopy reformed from the CT images has been recently attempted in many fields of medicine. We performed 3-dimensional virtual endoscopy to evaluate the patient's anatomy and the severity of IDD before treatment, and the findings were exactly the same as the operative findings. We propose that 3-dimensional virtual endoscopy is good alternative modality when the cause of duodenal obstruction is possibly due to the associated malformations of IDD and endoscopy cannot be performed or endoscopy has failed.
In conclusion, we report here on a patient with heterotaxia combined with IDD, and this was all successfully diagnosed and treated. We first used 3-dimentional virtual CT endoscopy for making the diagnosis and the treatment plan of this patient.



 XML Download
XML Download