

 PDF
PDF ePub
ePub Citation
Citation Print
Print


INTRODUCTION
Intimal hyperplasia (IH), also referred to as neointimal proliferation, is a major component of vascular remodeling and is responsible for the occlusion following angioplasty, stenting, endarterectomy, and bypass procedures.(1) Induction and progression of IH are thought to involve mechanisms related to wall shear stress (WSS), platelet aggregation/activation, the nature of the conduit, and neointimal proliferation after metabolic or stress-induced cellular injury, such as lipid disorders, hypertension, and tobacco use.(2-4)
Aortobifemoral bypass remains an important treatment for aortoiliac occlusive disease, despite the evolution in endovascular techniques.(5) In an aortobifemoral or aortobiiliac bypass, either end-to-end (ETE) or end-to-side (ETS) might be chosen for proximal anastomosis. In vitro studies have shown that, ETE anastomoses appear to offer a biomechanical advantage over ETS anastomoses with regard to WSS within the anastomotic region.(6,7) Experimentally, however, slow recirculation flow and the occurrence of anastomotic intimal thickening have also observed after ETE anastomosis.(8) Likewise, stenosis or occlusion at the proximal suture site of ETE anastomosis of aortobifemoral bypass is not infrequently observed as well as ETS anastomosis. We therefore compared the histomorphometric features of intimal remodeling after ETE and ETS anastomosis, the distribution of neointima between the bypass grafts and artery, and cytokine expression, in a rabbit model.
METHODS
In accordance with national laws on animal experiments, and with the permission of our university Ethics Committee, we utilized male New Zealand White rabbits, weighing 2.0~2.5 kg and aged 8~10 weeks (Orient, Sungnam, Korea). A total of 32 aorto-aortic bypass operations of 16 with ETS and 16 with ETE anastomosis were performed. Thirty operations were done using aortic grafts of 15 donor rabbits and 2 operations polytetrafluoroethylene (PTFE: Gore-Tex; W.L. Gore and Associates) grafts. To minimize bias from the immunologic response to aortic allografts or different graft size, a long aortic tissue obtained from one donor was divided into 2 pieces and shared between each of ETE and ETS bypass. PTFE graft bypasses, which are commonly used in clinical practice, were performed to provide comparison results for an allograft with a different compliance. Vessel wall changes were assessed at 1 day (n=1 per group), 5 days (n=1 per group), and 4 weeks (n=14 per group, including 1 per group operated with the PTFE graft).(9) Prior to harvesting of aortic segments, the rabbits were monitored daily, and their behavior, food and water intake, and neurological alterations were recorded.
1) Surgical technique
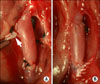
All animals were anesthetized with a combination of ketamine hydrochloride (10 mg/kg, Ketamine; Yuhan, Seoul, Korea) and xylazine hydrochloride (3 mg/kg, Rompun; Bayer Korea, Suwon, Korea), and maintained unconscious with inhaled isoflurane (Aerane; Baxter, Deerfield, IL, USA).(10) After shaving the abdomen and disinfecting the skin, the animals were prepared and positioned, and a median 6 cm abdominal incision was made. In donor rabbits, the aorta was identified and exposed by sharp dissection, and its branches were ligated with 5-0 black silk. After completing dissection and mobilization of the aortic segment, heparin (120 U/kg) was given intravenously prior to aortic clamping. Each harvested aortic graft was washed with heparinized saline and stored at 4℃ in histidine-tryptophan-ketoglutarate solution. After skin closure with nylon 3-0, donor animals were euthanized in a CO2 chamber. In the ETS anastomosis group, an arteriotomy measuring approximately 3 mm in length was made at the ventral surface of the aorta. The donor aorta or a PTFE graft, measuring approximately 9 mm in length, was anastomosed to the recipient aorta, using 8-0 polypropylene sutures and a continuous suture technique (Fig. 1A).(9) Upon completion of the anastomosis, the distal end of the recipient's aorta was ligated and transected. The distance between the caudal end of the anastomosis and the ligated terminus was 3 mm. The distal end of the transected aorta was anastomosed to the end of the aortic graft. ETE anastomoses with 8-0 polypropylene sutures were performed between the proximal and the distal end using a conti nuous suture technique (Fig. 1B). The length of each graft was approximately 6 mm.
After restoring the blood flow, the abdominal incision was closed with a running 4-0 Maxon skin suture. Recovery was aided by use of ketorolac tromethamine (Tarasyn; Roche Korea, Seoul, Korea) for 3 days.
2) Harvesting and staining of the grafts
At 1~28 days after the surgical procedure, the animals were anesthetized as described above, and the skin incisions were reopened. On mobilizing the aorta, the upper abdominal aorta was tied off after assessment of bypass patency, and cannulated distally to prevent shrinkage from fixation. A segment of the aortic graft containing the anastomosis, and a 3~4 mm portion of control vessel on either side were dissected from the surrounding tissues, and fixed for further histological assessment. After skin closure with nylon 3-0, the animals were euthanized in a CO2 chamber. The surgery sites were macroscopically assessed for stenoses and thrombi around the anastomosis, and sites where such features occurred were noted. Segments were stained with hematoxylin-eosin (H-E) or van Gieson stain for morphological evaluation of the anastomoses, identification of inflammatory cells and visualization of hyperplasic changes in the neointima. The neointima-to-media volume ratio was also quantified using imaging software (ImageJ; NIH, Bethesda, MD, USA).(11)
Anti-mouse proliferative cell nuclear antigen (PCNA) (clone PC 10, 1:1,000 dilution) (Sigma Chemical, St. Louis, MO, USA) and anti-mouse tumor necrosis factor-alpha (TNF-α) (dilution, 1:1,000) (Cell Signaling Technology Inc., Danvers, MA, USA) antibodies were used for immunohistochemical analyses. After blocking of endogenous peroxidase activity with 0.5% hydrogen peroxide in methanol for 5 min at room temperature, specimens were preincubated for 30 min with 10% goat serum in phosphate-buffered saline for 30 min, and then incubated at room temperature for 30 min with monoclonal antibodies against PCNA and TNF-α. Each vessel wall was divided into eight equal sections, and all cells within the media and intima were examined. Nonspecific cytoplasmic staining without nuclear involvement was considered negative. The PCNA labeling index was determined by dividing the number of PCNA-positive nuclei by the total number of nuclei in the neointima and media from each section. The intensity of anti-TNF-α staining of the intima and media of the eight randomly chosen sections was measured using imaging software (ImageJ). The medial and neointimal volume, PCNA indices and mean gray scale of TNF-α staining of the two groups were compared.
3) Western blot analysis
TNF-α and PCNA expression in three pair of bypass grafts explanted 4 weeks after surgery was analyzed by Western blotting. Each aortic segments bearing proximal anastomosis of 2 cm in length were snap-frozen, ground into powder, and lysed in 1 ml of 10 mM Tris-HCL (pH 7.4) containing 150 m-mol/L NaCl, 1% Triton X-100, and 1 mM phenylmethylsulfonyl-fluoride. The lysates were centrifuged and the supernatants subjected to sodium dodecyl sulfate-polyacrylamide gel electrophoresis, followed by transfer to nitrocellulose membranes, and incubation with anti-mouse TNF-α (dilution, 1:1,000) (Cell Signaling Technology Inc.) and anti-mouse PCNA (clone PC 10, 1:1,000 dilution) (Sigma Chemical) antibodies. Expression was quantitated using imaging software (ImageJ).
4) Statistical analysis
Intima and media thickness and volumes were compared using the Mann-Whitney U-test. Statistical analysis was performed using the statistical package SPSS for Windows (Version 12.0, SPSS Inc., Chicago, IL, USA). Statistical significance was defined when a P-value of <0.05 was obtained.
RESULTS
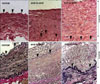
There was no graft occlusion or limb ischemia during 4 weeks of follow-up. Four weeks after bypass, the intimal proliferation were clearly recognized by H-E and van Gieson's staining (Fig. 2). The intima became thicker and had higher cellularity with typical spindle-shaped cells, and cellular proliferation around the suture thread disappeared. Whereas the neointima in ETE anastomoses were concentric, we observed a thick cellular layer, containing abundant extracellular matrix, on the ventral surface and heel of grafts that employed ETS anastomoses (Fig. 3).
Table 1 summarizes the light microscopy results for intimal thickness and volume. The thickness, area, and volume of neointima differed significantly between the two groups. Mean intimal thickness (0.883±0.048 mm vs. 0.721±0.047 mm) and mean neointimal volume (9.068±0.462 mm3 vs. 5.734±0.387 mm3) were significantly greater in the ETS group (P<0.05 for each comparison) (Fig. 2). Mean medial volume was, however, similar in the ETE (8.309±0.378 mm3) and ETS (8.446±0.316 mm3) groups. Using PTFE grafts, the neointimal maximal thickness and volume were 0.12 mm and 1.11 mm3, respectively, in the ETE group, and 0.84 mm and 3.62 mm3, respectively, in the ETS group (Fig. 4). Similarly, the intima/media volume ratio (0.70±0.05 vs. 1.08±0.06) was significantly smaller in ETE than in the ETS group (P<0.05). The circumference (15.853±0.306 mm vs. 24.877±0.817 mm) and area (15.364±0.382 mm2 vs. 24.419±1.157 mm2) of the lumen were significantly larger in the ETS than in the ETE group (P<0.05 for each comparison), but the intimal volumes of distal anastomoses did not differ significantly (7.63±0.042 mm3 vs. 7.98±0.030 mm3, P>0.05).
Immunohistochemical staining for PCNA and TNF-α showed a significant increase in the number of proliferating cells in the neointima of ETS grafts compared with the ETE anastomosis group. The PCNA index in the intima and media was also significantly lower in the ETE than in the ETS anastomosis group (6.01±2.01% vs. 17.22±6.12%, P<0.05) (Fig. 5). The intensity of TNF-α staining, calculated by use of a mean gray scale, was significantly weaker in the ETE group (150.29±6.57 vs. 125.67±3.12, P<0.05) (Fig. 5).
Western blotting of extracts of three entire bypass grafts 4 weeks after surgery showed significantly lower PCNA (152.66±7.37 vs. 175.53±4.36) and TNF-α (203.15±5.29 vs. 494.49±6.11) in the ETE group (Fig. 6).
DISCUSSION
Late graft failure caused by progressive IH is a persistent complication in arterial reconstruction, with IH accounting for 30~50% of bypass graft failures.(12) Implantation of a vein or prosthetic graft in the arterial circulation induces various changes that may lead to IH, including increased shear stress, loss of endothelial cells, migration and invasion of inflammatory cells, and migration and proliferation of vascular smooth muscle cells (VSMC).(13)
Pathologically, stenotic lesions after graft bypass have been shown to consist of VSMC proliferation with consequent luminal narrowing.(14) We assayed expression of PCNA and TNF-α to determine which cells had been stimulated to undergo proliferation. We found that medial VSMC proliferation occurred more when the ETS rather than the ETE anastomotic method was employed.
Activated leukocytes are an important trigger of VSMC proliferation in the development of luminal stenosis and occlusion. One of the cytokines strongly implicated in VSMC proliferation is TNF-α, an important mediator of both systemic and local inflammatory responses to vascular injury, and responsible for VSMC proliferation in a variety of settings including bypass surgery, arterial balloon injury and acute cardiac rejection.(15) In vitro, TNF-α induces adhesion molecule expression, promotes monocyte cytokine release, and stimulates VSMC proliferation.(16) In vivo, TNF-α has been causally linked to IH in vein graft and low-shear-stress models.(15,17) We observed significant differences in PCNA and TNF-α expression, by both immunohistochemical staining and Western blotting, between ETS and ETE anastomoses.
Since the aortic allografts in our model had good compliance, the effects of mismatched compliance and consequent angulation between the graft and host arteries were likely minimal. Therefore, we compared the pathologic findings of aortic allografts to those of the PTFE model, and the results were consistent. An abrupt increase in luminal size caused by ETS anastomosis, as shown by measuring the circumference and area of the lumen, may have resulted in the observed between-group difference in the degree and morphology of IH; the lesions were eccentric, and thickest on the ventral portion, in ETS anastomoses, but concentric in ETE anastomoses. This finding suggests that angulation of the anastomosis may have caused flow disturbance and subsequent IH. These data also suggest that ETS may have increased proliferative activity around the anastomosis and such anastomoses may be more prone to stenosis than are ETE anastomoses, and that both flow pattern and direction are important in late-phase IH formation. However, proximal anastomoses did not affect the degree of IH at distal anastomoses, and the anastomotic method seemed to have only a localized impact on the development of IH. At the same time, these changes were confined to sites near the anastomosis, suggesting that they were not related to an immunologic reaction to the allograft.
Although we found that ETE was superior to ETS anastomosis in reducing the rate of IH, clinical results have been mixed. Whereas some studies reported higher patency rates for ETE anastomosis after aortobifemoral or aortobiiliac bypass,(5,18) others found no difference.(19,20) ETE anastomoses have the theoretical advantage of less turbulence at the anastomosis; furthermore, the graft does not protrude anteriorly against the duodenum, and the graft limbs are less likely to kink. ETE anastomosis was considered preferable, in that angulation at the origin of the limbs of the prosthesis was found in ETS grafts.(21) In addition, the distal aorta, as the most common site for aneurysms and a potential source of emboli from ulcerated plaques, can be excluded.(22) The advantages of ETS anastomosis include technical simplicity and preservation of the inferior mesenteric artery; moreover, if graft occlusion occurs, there may be sufficient flow through the iliac arteries to prevent limb loss.(18) Furthermore, there may be an increased risk of impotence following ETE anastomosis.(22) Therefore, when choosing of proximal anastomotic method in arterial occlusive disease, the clinical parameters, including patient age, side branches near the anastomosis, and luminal size and appearance of the artery at operation should be considered with the surgical method associated with longer graft patency, at the same time.
We have developed an aortic bypass model in rabbits by interposing aortic allografts into the abdominal aorta using different anastomotic methods. The aorta used for both allografts and bypass sites had very thin intima, and changes in endothelial cells soon after surgery were difficult to detect by light microscopy. However, abundant intimal proliferation was readily visualized within 4 weeks. In addition, the aorta of a rabbit aged 8~10 weeks is approximately 2~2.2 mm in diameter and can be readily handled using a surgical loupe. Moreover, the anastomoses could be performed with running sutures.(9) Furthermore, ETE anastomosis was possible without raising concerns regarding distal organ ischemia, including colon and limb ischemia or paraplegia if the bypass was performed on the distal aorta near the bifurcation.
In conclusion, at 4 weeks, neointima developed mostly around the ventral surface in the ETS anastomosis group and circumferentially in the ETE anastomosis group. ETE anastomosis yielded significantly better results than did ETS anastomosis with respect to decreased IH, and may therefore improve long-term graft patency.





 XML Download
XML Download