

 PDF
PDF ePub
ePub Citation
Citation Print
Print


INTRODUCTION
Cyclosporine (CsA) and tacrolimus are the most widely used immunosuppressants for the prevention of acute organ rejection. However, due to their activity as calcineurin inhibitors (CNIs), CsA and tacrolimus cause hypertension, reduction of glomerular filtration rates, and chronic allograft nephropathy.(1,2) Given the negative side effects associated with CNIs, particularly nephrotoxicity, a potent non-CNI immunosuppressant has the potential to prolong allograft survival, as well as improve allograft function.(3,4) Sirolimus (SRL) has demonstrated potent anti-rejection activity and the ability to prolong allograft survival.(5) SRL has been reported to act synergistically with CsA in the reduction of acute rejection.(6) In a previous study, the addition of SRL to CsA and steroids significantly reduced the incidence of acute graft rejection in renal allograft recipients compared with the control regimen of CsA and steroids.(7) Direct SRL versus CsA comparison studies demonstrated that SRL has a different safety profile. In the SRL arm of the trial, better renal function, less hypertension, and fewer tremors were observed; however, SRL was associated with greater incidences of hyperlipidemia, leukopenia, and thrombocytopenia. Taken together, data from phases II and III trials suggest that SRL permits a low acute rejection rate when used with CsA and that the use of SRL as a base therapy without CsA may spare patients from the attendant toxicities of CsA. Therefore, in this study, we evaluated the efficacy of SRL-based immunosuppression therapy after early CsA withdrawal, as assessed by the incidence of biopsy-proven acute rejection episodes at 6 months, the safety of SRL, and graft function and survival over 12 months after transplantation in primary renal transplantation recipients in Korea.
METHODS
1) Patients and study protocol
This phase lllb prospective observational clinical trial was an open label, non-comparative, single treatment arm, multicenter study which was performed for 12 months. This study enrolled end-stage renal failure patients who were scheduled to receive a primary renal allograft from a deceased donor, a living-unrelated donor, or a living-related (excluding 0 antigen mismatch) donor from nine transplantation centers in South Korea between March 2007 and December 2007. A government-run Korean Network for Organ Sharing approved each transplantation surgery.
The number of patients was calculated by the formula under the assumption that binary variable approximately had a normal distribution for large patients.(8)
Using the formula, the needed sample size was 55 patients. Approximately 70 patients were planned to be enrolled in the study, considering 20% drop-out rate. We recruited 81 patients to ensure a sufficient number of patients for analysis.
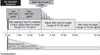
SRL treatment was initiated within 48 hours after transplantation, and was administered for up to 12 months (Fig. 1). CsA treatment was initiated before transplantation or within 48 hours after transplantation unless it was withheld by local practice for acute tubular necrosis or delayed graft function. Corticosteroids therapy was initiated within 24 hours before or after transplantation. Corticosteroids were administered by local standard practice at each study center, and tapered to a minimum of 5 mg/day of prednisone orally (or its equivalent) by the end of week 13. Withdrawal of corticosteroids was prohibited. All patients received SRL, CsA, and corticosteroids for 3 months after transplantation. At 3 months (±4 weeks) following transplantation, CsA was progressively withdrawn over 4 to 8 weeks while SRL was adjusted to obtain whole blood trough concentrations within 15~30 ng/ml (IMX®, Abbott, Abbott park, IL, USA) up to 6 months and within 12~24 ng/ml between 7 and 12 months (Fig. 1). When SRL and CsA were co-administered, SRL was administered approximately 4 hours after the morning dose of CsA; after CsA withdrawal, SRL was administered in the morning. This trial was approved by the institutional review board of each participating transplantation center, and it was monitored internally and externally.
2) Efficacy assessments
The primary efficacy endpoint was the incidence of biopsy-proven acute rejection episode at 6 months after transplantation. Renal biopsy was taken when acute rejection was suspected. For patient management, the interpretation of the pathologist at each site was used to define acute rejection according to the Banff 97 criteria for classification. Secondary efficacy endpoints included graft function at 6 and 12 months after transplantation (as determined by serum creatinine and e-GFR by Nankivell equation(9)) and patients and graft survival at 6 and 12 months after transplantation. The analysis of the data was based on an intention-to-treat (ITT) analysis. The summary of statistical analysis reported the number of patients with suspected and actual acute rejection events and the number of events per patient. This summary presented overall and monthly figures and figures for other appropriate time intervals. The percentage of patients with acute rejection over 6 months was reported along with corresponding 95% 2-sided confidence interval.
3) Safety assessment
Patients who received at least one dose of SRL were included in this analysis. All of the observed adverse events (AEs) were properly categorized, and then occurrence rates and confidence intervals were calculated. AEs were classified by using the Medical Dictionary for Regulatory Activities (MedDRA) 10.1.
RESULTS
1) Patient characteristics
A total of 81 patients were enrolled, but 2 patients were immediately excluded before transplantation due to cancellation of surgery (n=1) and withdrawal of consent before surgery (n=1). The remaining 79 patients who received kidney from living-related (n=63), living-unrelated (n=9) or deceased (n=7) donors composed the ITT analysis population. Of 79 patients, 59 (74.7%) completed medication for 12 months per protocol. Fifteen patients discontinued SRL before CsA withdrawal, and 5 recipients stopped the treatment after successful CsA withdrawal. Most common causes of SRL discontinuation were graft rejection (n=8) and protocol violation (n=3). Our patient demographics are presented in Table 1. Among them, 47 (59.5%) were female, and 32 (40.5%) were male. All patients were Korean. CsA withdrawal was initiated a mean of 96.1±14.2 days after transplantation, and 33.0±15.1 days were required to complete CsA withdrawal.
2) Dose and trough levels of immunosuppressive drugs
The mean daily dose and trough concentrations of SRL and CsA were summarized in Fig. 2. One week after CsA withdrawal, the mean SRL trough level was 15.8±5.2 ng/ml. At 4 weeks after CsA withdrawal, it was 16.2±4.2 ng/ml.
3) Efficacy evaluations
The incidence of biopsy-confirmed acute rejection episodes at 6 and 12 months after transplantation was 15.2% and 19.0% respectively 79 recipients. No subject had more than 2 acute rejection episodes. Eleven episodes were reported before CsA withdrawal and 1 episode after CsA withdrawal. The mean e-GFR at 6 and 12 months after transplantation was 67.4±15.3 ml/min and 71.9±18.8 ml/min respectively in the 79 ITT set. The mean serum creatinine level at 6 and 12 months after transplantation was 1.3±0.4 mg/dl and 1.3±0.4 mg/dl respectively in the 79 ITT set. There were no graft losses except ones due to patient death, with no causal relationship between graft loss and the study drug as determined by the investigator. The patient and graft survival rate at 12 months after transplantation was 97.5% and 96.2% respectively.
4) Safety evaluation
All patients reported at least one episode of AE. Among them, 78.5% patients reported 143 episodes of infection. The incidence of AEs related to the study drug was 91.1%, and infections related to the study drug were 46.8%. By system organ class using MedDRA 10.1, gastrointestinal disorders were most frequently reported in 66 patients (83.5%). The most frequently reported AE other than infection, was constipation (38.0%), serum cholesterol elevation (36.7%), and diarrhea (27.9%). Simple upper respiratory tract infection was the most common type of infection. SAEs were reported in 39 patients (49.4%). The most frequently reported SAEs were elevated serum creatinine concentration (12.7%), lymphocele (7.6%), herpes zoster infection (7.6%), and pulmonary infection (6.3%). Seven SAEs (5 lymphoceles, 1 ventral hernia, and 1 wound seroma) with wound healing were reported, and the investigators concluded that only 5 SAEs were related to SRL.
Hematology and blood chemistry, lipid profile of patients are presented and summarized in Table 2. There was a change during study period. However, most hematologic test results were within normal ranges, and no clinical toxicity was observed. The cholesterol level was 160.09±35.91 mg/dl at screening and 224.63±43.41 mg/dl at 12 months after transplantation. The mean triglyceride level was 122.91±67.88 mg/dl at screening stage, 189.63±99.73 mg/dl at 12 months after transplantation.
DISCUSSION
This is prospective observational and first pilot study about the efficacy and safety of SRL in Korean renal transplantation recipients. However, the study population was relatively smaller than previous study performed in other countries. This study is originally planned and performed as a pilot study before commercial use of SRL. In Korea, SRL is not supported by the National Medical Insurance Program. So, study population cannot use SRL as a main immunosuppressant freely after study period. This point is one of the limitations in the SRL use and expanding study population.
The use of SRL has been directly compared to that of CsA in two phase II trials for the prevention of acute rejection in renal allograft recipients. In these studies, SRL was shown to have efficacy similar to CsA in preventing acute graft rejection, although the observed acute rejection rates were higher than those obtained with the SRL-CsA combination.(10,11) The incidence of acute rejection confirmed by biopsy within 6 and 12 months in this study was 15.2% (12/79) and 19.0% (15/79) respectively. This result is similar to 17.2% (37/215) and 20.0% (43/215), in the same order, found in the previous study in other countries.(4) Most episodes of acute rejection occurred before CsA withdrawal. Only 3 episodes of acute rejection occurred after CsA withdrawal. We can confirm that our efficacy and safety profiles are similar to those of the previous study.
During the study period, 3 patients died with no causal relationship to the study drug. A 49-year-old male died from asphyxia one month after. A 50-year-old male was found dead in his house 7 months after study medication began. There were no AEs reported in this patient. Cause of death was presumed as a myocardial infarction according to his medical record. A 58-year-old female who started the study medication on November 6, 2007, stopped on November 26, 2007 due to thrombocytopenia and pneumonia. She died from myocardial infarction on January 16, 2008. While the investigator concluded that her thrombocytopenia and pneumonia was related to SRL, but the myocardial infarction was not related to SRL.
Based on this study, CsA and SRL induction followed by CsA withdrawal at 3 months post-transplant is considered to be efficient and safe after primary renal transplantation. SRL maintenance regimen has been shown to be an effective treatment for the prevention of renal acute rejection episodes in primary renal allograft recipients.



 XML Download
XML Download