

 PDF
PDF ePub
ePub Citation
Citation Print
Print


INTRODUCTION
Adhesions, defined as the abnormal joining of two normally separate tissue surfaces, are a natural consequence of the normal healing response. After laparotomy, almost 95% of patients are shown to have intraperitoneal adhesions at subsequent surgery.(1) These can result in intestinal obstruction, secondary infertility, chronic abdominal or pelvic pain, and complicated and difficult subsequent operations. Moreover abdominal adhesions have major financial implications. In 1994, adhesion-related health care costs in the United States were estimated at US $1.3 billion.(2)
Although a variety of surgical techniques and agents have been advocated to reduce the formation of postoperative adhesion,(3,4) the use of physical 'barriers' that minimized any apposition of serosal surfaces during the critical period of mesothelial repair remained the preferred technique. There were two absorbable antiadhesive barriers, Interceed® (Johnson & Johnson, Sommerville, NJ, USA) and Seprafilm® (Genzyme Corporation, Cambridge, MA, USA), which were approved by U.S. Food and Drug Administration (FDA).(5) Interceed® is composed of oxidized regenerated cellulose and a gelatinous material slowly absorbed from the peritoneal cavity over 28 days, which efficacy and safety has been shown in a prospective randomized clinical trial.(6-8) Seprafilm® is a bioresorbable membrane derived from sodium hyaluronate (HA) and carboxymethyl cellulose (CMC), which turns into a gel approximately 24 hours after placement and remains in place for up to 28 days. The benefit of Seprafilm® has been demonstrated in preclinical and clinical trials.(9-11)
However these membranes were not easy to apply topically or laparoscopically.(5) So a solution form, a mixed solution of HA and CMC, was developed to be easily spread and widely coated.(12,13) This injectable solution can be used in laparoscopic surgery, but it is possible to run down from targeted area to the bottom of the peritoneal cavity and to fail to show antiadhesive effect on that area. In the effort for development of innovative injectable materials to stay on targeted area, thermosensitive poly (organophosphazene) hydrogels have been introduced.(14) These aqueous polymer solutions are biocompatible and reversibly transformed into hydrogels at body temperature, and display hydrolytic degradation properties.(14,15)
The aim of this study was to compare the efficacy of two injectable antiadhesive agents- the thermosensitive poly (organophosphazene) hydrogel and the mixed solution of hyaluronate and carboxymethyl cellulose- with that of the membrane agent (one established agent [Interceed®]) and control (phosphate buffered saline).
METHODS
1) Materials
The thermosensitive poly (organophosphazene) hydrogel have a polymer backbone containing hydrophobic isoleucine ethyl esters (IleOEt), hydrophilic α-amino-ω-methoxy-polyethylene glycol (AMPEG) and hydrolysis-sensitive glycyl lactate ethyl ester (GlyLacOEt) as substitutes. These substitutes are related to controllable hydrogel characteristics such as gelation temperature, gel strength, and biodegradability. In this study, [NP(IleOEt)1.46(GlyGlyCOOH)0.06(AMPEG750)1.08]n was synthesized according to published methods with permission.(14) An aqueous polymer solution was prepared, dissolving 2 g of the polymer in Phosphate buffered saline (PBS, 0.01 M, pH 7.4) by continuous stirring at 4℃ for 3 days. The polymer solution (8 wt.%) was filtered using Millipore filters (Millipore, Madison, WI, USA, diameter 0.45µm) and sterilized with ultraviolet radiation over 6 hours. The solution was stored in sterile 1 ml syringes at 4℃. Guardix-sol®, which is a mixed solution of 0.25% (w/v) hyaluronate and 0.49% (w/v) carboxymethyl cellulose, was purchased from Hanmi Inc. (Seoul, Korea). Stock 10 ml solutions in a 10 ml Luer lock syringe were divided and stored in sterile 1 ml syringes. Twelve 2×5 cm sized pieces of Interceed® were prepared as the positive control from two purchased sterile 7.6×10.2 cm-sized sheets from Johnson & Johnson (Langhorne, PA, USA). PBS (0.01 M, pH 7.4) was used as the negative control.
2) Animals
Twenty-four male Sprague Dawley rats (310~410 g; Orient Bio Inc.) were used to induce adhesions. They were individually housed at a constant room temperature and humidity, with 12:12 h light and dark cycles, and were provided food and water ad libitum throughout. All animal experiments were performed at the Department of the Laboratory for Experimental Animal Research in the Clinical Research Institute at Seoul National University Hospital (AAALAC International accredited facility). The approval of the Institutional Animal Care and Use Committee (IACUC) was received, and National Research Council (NRC) guidelines for the care and use of laboratory animals were observed (revised 1996).
3) Induction and management of adhesions
The ischemic button model using rats was chosen for comparison of anti-adhesive effect. In the ischemic button model using rats, eight buttons were created in one rat and adhesions on the button were analyzed, which makes this model require smaller number of rats. Moreover it is a standardized qualitative and quantitative model and has been shown to provide reproducible results and constant adhesion formation.(16,17) Reed et al.(17) reported that in control group with normal saline, the 72.2 (±4.7) to 82.0% ischemic buttons of Wister rats formed adhesions attached to various structures in the peritoneum including liver and small bowel after 1 week.
Peritoneal adhesions were created in rats as described. (16,17) After isoflurane inhalation anesthesia, each rat's weight was checked, and the abdomen was shaved and swabbed with 70% alcohol. A laparotomy was performed through a 5 cm midline incision. Four ischemic buttons, spaced 1 cm apart along the paracolic gutter, were made on both sides of the parietal peritoneum by grasping 5 mm of peritoneum with a hemostat and ligating the base of the segment with a 4-0 silk suture (Fig. 1A). Twenty-four rats were randomized to four experimental groups managed with 1 ml of the aqueous polymer solution (the Gel group, n=6), 1 ml of Guardix-sol® (the Gd group, n=6), two 5×2 cm pieces of Interceed® (the IC group, n=6), or 1 ml of PBS (the control group, n=6). Then, the agents in a syringe were applied on all ischemic buttons or the membrane was applied to cover all ischemic buttons on both sides (Fig. 1B). The laparotomy incision was closed in one layer with 3-0 coated Vicryl*Plus® (Ethicon, Sommerville, NJ, USA) suture.
4) Assessment of adhesions
After two or four weeks, three rats in each group underwent a secondary laparotomy. The ischemic buttons were inspected for the presence or absence of adhesions to evaluate antiadhesive efficacy using the following measurements (Fig. 2)(18):
(1) The general overall health of the tested animals indicated by the percentage of their gained weight relative to basal weight.
(2) The extent of adhesions recorded as the number of the adhered buttons in a rat.
(3) The incidence of adhesion recorded as the existence of attached adhesion to each button in a group.
Two rats in the IC group were excluded because one rat had intraoperative mesenteric bleeding and required meticulous hemostasis and evacuation of hematoma, and the other died six days after initial surgery, and autopsy was not possible. Therefore, the number of adhered ischemic buttons was analyzed in the remaining 22 rats.
5) Tissue preparation and histology
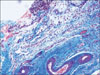
To analyze the histology of adhesion, peritoneal tissue from representative areas was obtained from one rat in each group under sterile conditions. It was fixed in buffered formalin (4%), embedded in paraffin, cut into 4 to 5µm sections and stained with hematoxylin and eosin under standardized conditions. Masson trichrome staining was used to demonstrate tissue fibrosis. All slides were analyzed using light microscopy (Olympus BX45, Olympus, Germany). Histological features including adipose tissue, collagen, fibrosis, and vascularization were analyzed by a pathologist.
6) Statistical analysis
All variables are expressed as the means with standard deviation. Differences among the four groups were evaluated by Kruskal-Wallis variance analysis, followed by a post hoc Mann-Whitney nonparametric U-test. Fisher's exact test was used to assess any differences in incidence. P<0.05 was considered statistically significant. All data were processed using SPSS version 12.0 (SPSS Inc., Chicago, IL, USA).
RESULTS
At the secondary laparotomy, there were no residual materials of antiadhesive barriers in any rats. And two rats in each group were found to have two or three loosened knots for ligating ischemic buttons, but this was considered not to be significant and was not analyzed.
1) Changes in weight
The mean basal weight of 22 rats was 349±24 g (range 312~410) and there was no difference between 4 groups (P=0.402). The mean percentages of gained weight in each group at two and four weeks were showed in Table 1 (Gel vs. IC, P=0.083; Gel vs. Gd, P=0.050, respectively).
2) The extent of adhesions
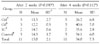
The mean number of buttons with adhesion in a rat in each group was showed in Table 2, and there was no significant difference between four groups at any time (P=0.084 after 2 weeks and P=0.197 after 4 weeks). When comparing between the mean number of adhered button in a rat after 2 weeks and that after 4 weeks, there was no difference in each groups. After the rats at two period were put together, the extent of adhesion in the IC group was significantly smaller than that in other groups (P=0.004). In addition, the Gel group also showed fewer adhesions than the Gel groups and the control group, although it was not statistically significant (P=0.074, and P=0.310, respectively).
3) The incidence of adhesions
The overall numbers of adhered ischemic buttons were significantly different between groups at two weeks (P=0.001) and at four weeks (P=0.003). After the rats at two period were put together, overall number of adhered ischemic buttons were 23 in the control group (n=48), 22 in the Gd group (n=48), 14 in the Gel group (n=48) and 0 in the IC group (n=32) and those of each group were significantly different (P<0.001). That of Gel group was significantly bigger than of the IC group (P=0.001) and it was smaller than the control group and the Gd group, although not statistically significant (P=0.093 and P=0.140, respectively). And that of Gd group was bigger than that of IC group (P<0.001) and not significantly different from that of the control group (P=1.000).
4) Histology
Characteristic acute and chronic inflammatory reactions caused by ischemia were observed around the sutures. There were dense infiltrations with mixed granulocytic and lymphoplasmocytic inflammatory cells with numerous multinucleated giant cells. However in the adhered tissue, there was no sign of acute inflammation, only slight lymphocytic infiltration without granulocytes or macrophages. Most of the adhesions examined consisted of varying amount of adipose tissue and tortuous vascularized bands of collagen. Loosely arranged collagen fibers of heterogeneous size were often found adjacent to regions of dense fibrotic tissue within the same adhesion (Fig. 3). There was no significant difference in each group at two and four weeks.
DISCUSSION
The ideal antiadhesive barrier, besides being effective and safe, should be noninflammatory, nonimmunogenic and biodegradable, and should stay in place during the critical remesothelialization phase without sutures or staples and remain active in the presence of blood. Although Interceed® as the established antiadhesive membrane in this study had demonstrated benefit for reducing the incidence and extent of adhesion, its effect was known to be decreased in the presence of blood resulting adhesion formation.(3,7,8) Moreover, the difficulty in manipulating and applying it during laparoscopic surgery limits its usefulness. Seprafilm®, which is derived of HA and CMC, showed antiadhesive effects in preclinical and clinical trials.(9-11) Although there were only a few studies on the mixed solution form of HA and CMC, it is expected to have similar antiadhesive efficacy as the membrane form and has specific advantages including easy spreading and wide coating.(12,13)
This study compared two injectable antiadhesive agents including a novel polymer with a membrane agent and controls. The mixed solution demonstrated no definite antiadhesive effect. It was possibly because the most solution ran down the both sides of the parietal peritoneum before firm coat on the ischemic buttons. If the solution were to change to a gel after application and were to remain separating the raw peritoneal surfaces, it could reduce postoperative adhesions. Therefore, adjusting the ratio of HA to CMC or further large-scale studies seems to be necessary. The poly (organophosphazene) hydrogel showed some antiadhesive effects. Although the aqueous polymer solution was expected to immediately change to gel at a rat's body temperature, its gelation took more than 15 minutes and some amount of solution ran down into the dependent portion of the rat's body. It was possible that gelation started at a location distant from the ischemic buttons. That implied that the gel requires precise control of hydrogel characteristics such as gelation temperature, gel strength and biodegradability. In terms of weight gain, that of the Gel group after four weeks was less than that of the other groups, which was not statistically significant, which implies that the gel is biocompatible as other agents.
This study analyzed the efficacy of the gel as adhesion barriers in an animal model that involves tying, which mimics clinical circumstances. The resulting adhesions were scored 2 and 4 weeks postoperatively, which is after the critical phase of 3~5 days during which adhesions can form.(19) Especially the time point of postoperative 2 weeks is also in keeping with most other studies of adhesion formation,(20) although it showed no histological difference with the time point of postoperative 4 weeks in this study. The ischemic button model using rats allows a standardized qualitative and quantitative measurement. (16,17) One possible weakness of this method might be that the model provides no information about the strength of adhesions. A further possible weakness of the model is that the percentage of ischemic buttons in the control (PBS) was lower than that of references group. In a control group with normal saline, 72.2% to 82.0% of the ischemic buttons in Wister rats had formed adhesions attached to various structures in the peritoneum including the liver and small bowel after one week. We did not analyze the difference between PBS and normal saline for different species of rats. In spite of these limits, this ischemic button model with rats is useful as it is objective, simple and easy to perform.
In conclusion, two injectable antiadhesive agents were developed to easily apply to targeted area and in laparoscopic surgery. However the mixed solution of CMC and HA failed to show the anti-adhesive effect. The poly (organophosphazene) hydrogel demonstrated some possibility of having an antiadhesive effect although most solution ran down into the dependent portion of the rat's body before gelation. Therefore the gel requires precise control and a large-scale preclinical study to verify these findings before application in laparoscopic surgery.



 XML Download
XML Download