

 PDF
PDF ePub
ePub Citation
Citation Print
Print


INTRODUCTION
In major surgery such as radical gastrectomy in gastric cancer patients, transurethral catheterization of the urinary bladder has been commonly performed for monitoring of the output amount during the operation and the early postoperative period. This long-term use of urinary catheterization has been empirically performed in most abdominal surgeries without acceptable evidence as it has been widely believed that it is necessary for prevention of acute postoperative urinay retention (APOUR), monitoring of urine output, and serves as a marker of hemodynamic stability.(1) However, there are several disadvantages such as urinary tract irritation, pain, increased urinary tract infection (UTI) risk, delayed recovery of bladder function, inconvenience of foreign body sensation, disturbance of postoperative early ambulation, and embarrassment during recovery periods.(2,3) The adequate indications and optimal duration of bladder catheterization remains controversial.
Recently, with an increase in enhanced recovery after surgery (ERAS) program or fast-track surgical procedures, transurethral catheterization is limited to fewer procedures, for a shorter time. Patient discomfort and early return to daily activities are factors that are sometimes not considered by the physicians when making the decision whether to perform the indwelling catheter. For improving patients' tolerance of surgical trauma, early removal of the indwelling catheter is recommended in the ERAS program. In this aspect, unneccessay urinary catheterization for long periods is a major disturbance for early recovery.(4,5) In particular, anxiety for aggravation of urinary tract pain at ambulation and intricate transurethral catheter system including the collection bag are important disturbance.
For restriction of transurethral catheterization, the most serious clinical problem is APOUR. So, awareness and selection of patients at risk of developing APOUR would be of great significance. It has been suggested that bladder catheterization should be advised in high-risk subjects when the bladder volume is greater than 600 ml over a minimum period of 2 hours.(1)
Our hypothesis is that empirical long-term use of transurethral bladder catheterization is not mandatory for all patients undergoing radical gastrectomy. Recently, radical gastrectomy is not considered to be high risk surgery any more, because the duration is not long, and massive bleeding during surgery is rare. In this study, we aimed to evaluate the feasibility of immediate removal of transurethral catheter in hemodynamically stable patients undergoing radical gastrectomy, prior to a prospective randomized controlled trial (RCT).
METHODS
1) Study setting
This feasibility study was performed at a single institute. All patients gave their written consent for this study after receiving a full explanation of the study including the purpose, potential benefits and complications.
2) Patients
A total 63 gastric cancer patients undergoing elective radical gastrectomy in Seoul St. Mary's Hospital were enrolled for feasibility study. A complete history and physical examination were undertaken for all possible candidates to determine eligibility for inclusion. There were no specific inclusion or exclusion criteria for this feasibility study, but a total 5 patients were excluded for safety reasons. The reasons of exclusion were old age (over 75 year old; n=2), high prostate-specific antigen (PSA) level (n=2), severe chronic disease (liver cirrhosis-child B; n=1). There were no hemodynamically unstable patients needing intensive care unit (ICU) care after radical gastrectomy in the included patients.
A total 58 patients were included in this study. In the process of the study, 6 cases were dropped out in active group, and 2 cases were dropped out in control group. Finally, 25 patients were included for analysis in both groups, respectively (Fig. 1).
3) Patient grouping and protocols according to groups
All patients were randomized to either active group (immediately removal group) or control group (removal at postoperative day 1 group). Patient's blinding was undertaken within this feasible study design.
All transurethral catheterizations (Foley® catheter, SEWON medical, Co. Ltd., Cheonan, Korea) were performed by the surgeon or surgical resident after induction of general anesthesia. The transurethral catheter was introduced after disinfection (povidone-iodine) of the skin around the meatus of the urethra followed by moisturizing the catheter tip and distal urethra with lubricants.
Patients in active group had the transurethral catheters removed immediately before going to the postanesthesia care unit (PACU). During 24 hours after operation, patients in active group were frequently encouraged about timed-self voiding every 4 hours by physician or nurse, and residual urine (RU) was checked by using a portable bladder ultrasound device every 4 hours. If the RU checked was over 400 ml, the nurse encouraged self voiding for 30 minutes regardless of voiding sense with questions about subjective suprapubic discomfort or voiding sensation. Thereafter, if there was no self-voiding for 30 minutes, in-out transurethral catheter (Nelaton® catheter, SEWON medical, Co. Ltd., Cheonan, Korea) drainage was performed immediately regardless of voiding sensation for patient's safety. However, when the patient complained suprapubic discomfort or distension, in-out transurethral catheter drainage was also performed immediately for safety. Moreover, if the number of in-out transurethral catheter drainage was over 2 times, recatheterizations by transurethral catheter (Foley®) was performed, and the patient was dropped from the study. The other indications of drop-out were major postoperative complications which needed monitoring of the urine output or relaparotomy.
Patients in control group had the transurethral catheter removed the morning after surgery (postoperative day [POD] 1) according to established protocol.
Postoperative fluid was administrated according to standard protocol in both group, that total 2,000 ml was infused regularly for 24 hours (infusion speed, 83 ml/hr) in cases below body mass index (BMI) 23 kg/m2, and total 2,500 ml was infused regularly for 24 hours (infusion speed, 104 ml/hr) in cases over BMI 23 kg/m2.
4) Measurement of outcomes
APOUR was generally defined as undergoing in-out transurethral catheter drainage or recatheterizations with transurethral catheter. RU was checked by using portable bladder ultrasound devices (scale; ml). Operative factor included the operation time (from endotracheal intubation to extubation), amount of infused fluid (crystalloid and colloid fluid), amount of mesured urine (urine output), and amount of lost blood (blood loss). The first voiding discomfort level was measured by visual analog scale (VAS) score. Urinary discomfort was measured by a structured questionnaire (including 5 questions; urinary pain, burning on urination, frequency, urgency, and residual sensation) using the McGill Pain Questionnaire at POD 2, and the measured score recorded categorically (no, 0; scanty, 1; some, 2; moderate, 3; very, 4), and reclassified into 2 categories (0~1, negative; 2~4, positive) for statistical analysis.(6) The urine analysis was performed at POD 5 before discharge by dipstick exam and bacterial culture with first voiding mid-stream urine. Hematuria and pyuria was defined as results of more than trace in dipstick exam, and bacteriuria was defined as the presence of over 100,000 of any microorganism per ml urine on culture. The results of urinary analysis before discharge were compared with the results of preoperative urinary analysis, and positive finding was represented a case which was newly developed state in postoperative urine analysis.
5) Statistics
This study was designed to confirm feasibility. The results of the continuous variables are expressed as means±standard deviation (SD). Univariate statistical analysis was performed using Mann-Whitney U test for continuous independent samples, and Chi-square or Fisher's exact test for the categorical variables, respectively. Statistical analyses were performed using SPSS software (Ver. 13.0) and a P-value<0.05 was considered to indicate a statistically significant difference with a 95% confidence interval (95% CI).
RESULTS
There were no significant differences between the 2 groups regarding age, sex, and operative factors (Table 1).
In the process of the study, 6 cases were dropped out in active group, and 2 cases were dropped out in control group, respectively. These 8 patients were diagnosed with APOUR according to our criteria. The incidence of APOUR was 19.4% in active group (6/31), and 7.4% in control group (2/27), respectively.
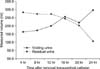
In the active group, the mean volume of self-voiding after 4 hours was 164 ml, and RU measured was 283 ml. The self-voiding volume increased gradually, and the residual volume decreased over time. However, the self-voiding and RU volume was measured nearly equal (256 ml vs. 244 ml) 16 hours after transurethral catheter removal, and showed difference of volume after 24 hours (Fig. 2).
Regarding the degree of first self-voiding discomfort after removal of transurethral catheter, there were significant differences between the 2 groups. The VAS score (degree of first self-voiding discomfort) was lower in active group compared to control group (P=0.041) (Table 2).
Regarding the urinary discomfort at POD 2 and the urine analysis at POD 5, there were no significant differences between the 2 groups (Table 2).
DISCUSSION
For improving patients' tolerance of surgical trauma, early removal of the indwelling catheter and early ambulation is recommended in the ERAS program.(4,5) In this aspect, unneccessary urinary catheterization for long periods would be a major disturbance for early recovery. The major goal of bladder catheterization is the prevention of APOUR. It must be necessary, for it serves as a marker of hemodynamic stability during operation, but there have been controversies for the long-term use in recovery periods due to several disadvantages such as severe pain of urinaty tract, foreign body sensation, disturbance of postoperative early ambulation, and embarrassment. In particular, fear of urinary tract pain at ambulation is a major disturbance for early ambulation, and the intricate transurethral catheter system including the collection bag is another important disturbance. Moreover, most patients felt shame at the general ward. In the postoperative period, the urinary output will be decreased in the fast-track program, because the volume of intravenous fluid is restricted to induce early recovery of bowel function.(7,8) The restriction of unnecessary urinary catheterization could be helpful for early recovery program after surgery, if APOUR could be prevented or detected early. However, there have been no results about the usefulness of transurethral bladder catheterization in major upper abdominal surgery.
In recent reports, the risk factors of APOUR were presented. Preoperative factors are age (more than 50 years old), male gender, lower abdominopelvic surgery, preexistent urinary disease (especially benign prostate hyperplasia, BPH), and previous pelvic surgery. And, intraoperative factors are large amount of intravenous fluid in lower abdominal surgery, long duration surgery, and spinal or epidural anesthesia. Lastly, postoperative factors are bladder volume at PACU (over 270 ml) and postoperative analgesia.(1,9-12) However, radical gastrectomy in hemodynamically stable patients has not been included as risky surgery for APOUR any more, because it is not lower abdominopelvic surgery, the duration is not long, and no longer requires large volumes of intravenous fluid. In this studys, the duration of surgery was shorter than the presented risk factor (200.5±39.7 min in control group, 190.7±39.9 min in active group), and total amount of blood loss averaged less than 300 ml in both groups. Moreover, the urinary bladder could be completely emptied by bladder catheterization during operation. Therefore, we hypothesized that empirical long-term use of transurethral bladder catheterization is not mandatory for all patients undergoing radical gastrectomy, and decided to perform a prospective RCT for evidence. But, we also think that the age and gender factors should be controlled with adequate enroll criteria under the ethic point of view in RCT.
The overall incidence of APOUR has been reported to be between 14% and 30.2% regardless of the type of abdominopelvic surgery. One of the important reason of marked differences among the studies is that there have been controversies about the definition of APOUR.(12-14) In this study, the incidence of APOUR was respectively 19.4% in active group, and 7.4% in control group with our provisional criteria (A case which undergone in-out transurethral catheter drainage or recatheterizations with transurethral catheter). These results are comparable with other reported outcomes. In active group, 4 patients had transient in-out catheterization, and 2 patients had transurethral catherization. We think that the former (4 patients) resulted from relatively provisional lower criteria (RU was estimated to be over 400 ml in portable bladder ultrasound devices) for performing in-out catheterization compared with other previous studies. The adult urinary bladder has a capacity of 400 to 600 ml, and only 13% of patients required transurethral catheterization due to inability to void among the patients assessed with bladder ultrasound to have a bladder volume greater than 400 ml.(11) Moreover, it was presented that in-out catheterization should be recommended if the volume assessed by bladder ultrasound is more than 600 ml in high-risk patients.(1) Therefore, we think that the criteria for performing in-out catheterization should be revised adequately in RCT. The latter (2 patients) resulted from urethral injury during catheter insertion and administration of large amount volumes with injection of diuretics during operation (more than 4,000 ml), respectively. These factors, technical quality of transurethral catheter insertion and volume of intravenous fluid, also should be controlled in RCT.
The residual urinary baldder volume could be checked easily by portable bladder ultrasonic devices in the general ward as a diagnostic tool for APOUR. The bladder ultrasound device has been shown to provide an accurate assessment of urinary bladder volume and a guide to the management of APOUR.(15) In this studys, the difference between urinary volume measured by the portable bladder ultrasound and by in-out catheterization varies minimally (data not shown).
There have been no previous comparable results in respect to urinary discomfort after nonuse of urinaty catherization in upper abdominal surgery. However, it was reported that non-placement of indwelling urinary catheter during cesarean section was more convenient, with no urinary retention.(2) In this study, the discomfort score of first self-voiding after removal of transurethral catheter was significantly lower in active group compared to control group (2.5 vs. 2.0; P=0.041), but the score of urinary discomfort at POD 2 did not show differences.
UTI has been known to be a common complication of long-term transurethral catheter use. The incidence of catheter-related UTI varies from 8% to 21%.(1,16,17) It was reported that maximum 50% of the patients with a transurethral catheter have lately complained of persistent urethral burning and the desire to micturate.(4,18) Other authors also reported that catheter-associated UTIs are rarely symptomatic, often go untreated, and are associated with a large reservoir of antibiotic-resistant bacteria and yeasts.(19) In these studies, incidence of pyuria was below 15% in both groups without significant difference, and incidence of bacteriuria did not show significant difference. But, the incidence of bacteriuria was relatively high in both groups (20% and 32%, respectively) because there was cultured normal flora in women.
In conclusion, the results of this study showed that the immediate removal of transurethral bladder catheterization after radical gastrectomy could be safe and feasible in hemodynamically stable patients undergoing radical gastrectomy in aspect of ERAS program. The prospective RCT would be scheduled under the Institutional Review Board (KC09OISI0225) supervision for acceptable evidences.



 XML Download
XML Download