

 PDF
PDF ePub
ePub Citation
Citation Print
Print


INTRODUCTION
Bronchogenic cyst outside the thoracic cavity is a very rare and, in most cases, is described as retroperitoneal masses, result of incidental findings in the course of a computer tomography (CT). Pure intraabdominal locations are extremely uncommon.(1)
Congenital bronchogenic cysts are observed not only in infants and children, but also in adults. Although some bronchogenic cysts are asymptomatic,(2) they have potential complications, such as infection, bleeding, or malignization. These potential complications and the lack of a certain pathological diagnosis make surgical resection.(3)
CASE REPORT
We present a 20-year-old woman presented to our hospital with an incidentally detected gastric submucosal tumor, which was in gastric cardia. She has history of hospitalization for treatment for hepatitis A, 2 months ago. During her admission period, abdominal CT was performed for hepatic evaluation. And, gastric mass was detected incidentally. A physical examination demonstrated no palpable mass in the abdominal region. Laboratory values were normal. Diagnostic work-up including gastroduodenoscopy, endoscopic ultrasonography and abdominal CT revealed a 2 cm sized submucosal tumor, originate from gastric 4th layer in the cardia (Fig. 1). Gastrointestinal stromal tumor was considered preoperatively. Thus, partial gastrectomy was planned.
Via laparoscopic approach in the lesser gastric curvature, we observed a 2.5×2 cm sized cystic tumor (Fig. 2). It was originated in the gastroesophageal junction, and there was no communication with the esophageal and gastric wall. Laparoscopically, it was dissected from the gastric wall and resected with Harmonic Scalpel® (Ethicon Endo-Surgery, Cincinnati, OH, USA). We reviewed the rest of the gastric wall, and there are no serosal defects (Fig. 3). The postoperative course was uneventful, soft diet feeding start on postoperative day one. She has no passage disturbance and the patient was discharged on the second postoperative day.
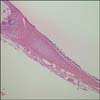
Histological studies of the surgical specimen revealed a cyst lined with stratified epithelium and surrounded by smooth muscle cell (Fig. 4), and the final diagnosis was of a bronchogenic cyst.
DISCUSSION
Bronchogenic cysts are the result of abnormal budding of the primitive tracheobronchial tube.(4) The location of the cyst depends on the embryological state of development at which abnormal budding occurred. They are usually intrapulmonary or mediastinal and are rarely located in unusual places, such as the cutaneous and subcutaneous tissues, neck, pericardium, diaphragm, abdomen, and the intramedullar part of the spine.(5) A preoperative diagnosis of bronchogenic cyst is difficult. CT shows the cystic nature of the mass. However, if the cyst is infected or high in protein and calcium, its density may fall into the solid-tissue range, which increases diagnostic uncertainty. Endoscopic ultrasound (EUS) is useful in the preoperative diagnosis of bronchogenic cyst.(6) In our case, gastric gastrointestinal stromal tumor was considered preoperatively. Because of endoscopic and EUS findings were gastric 4th layer mass and gastrointestinal stromal tumor is much more common than a congenital cyst. Endo-organ surgery is an important treatment option for these tumors because of the inability of endoscopic biopsy to obtain submucosal tissue. A definitive diagnosis and complete tumor excision up to 4 cm in diameter are possible with intraluminal surgery.(7) Thus, we originally planned to conduct laparoscopic intragastric resection. Following careful review of CT, we presumed cystic mass has exophytic lesion. Subsequently, we switched our plan and conduct extragastric wedge resection. As a result, we were able to properly operate, diagnose, and treat.
We performed minimal invasive surgery by leveraging the great visibility afforded by laparoscopic surgery. We reported an uncommon intra-abdominal bronchogenic cyst, which was completely resected via laparoscopic surgery.



 XML Download
XML Download