

 PDF
PDF ePub
ePub Citation
Citation Print
Print


Abstract
Purpose
The liver hanging maneuver (LHM) is a useful technique enabling a safe anterior approach, which is one of the most important innovations in the field of major hepatic resections. This study was conducted to review tumors' profiles after applying this procedure and to evaluate the usefulness of LHM and Glissonean pedicle transaction method (GPTM).
Methods
Medical records of 64 patients who underwent hepatic resection using LHM and GPTM at the Asan Medical Center were reviewed. The classic LHM was conducted according to the Belghiti method.
Results
Among 64 patients, 46 patients had hepatocellular carcinoma; 7, intrahpatic cholangiocarcinoma; 4, hilar cholangiocarcinoma; 4, metastatic liver cancer; 3, benign liver tumor. Mean tumor size was 10.6 cm (3~22). Mean liver parenchymal transection time was 20 min (15~30). Right side hepatectomy was performed in 44 patients; left side hepatectomy with or without caudate lobe was performed in 19 patients. Twenty patients (31.3%) required blood transfusion during surgery. There was no in-hospital mortality or major complications. Minor complications developed in 6 patients (9.37%).
Figures and Tables
Fig. 1
Various hepatectomy using hanging maneuver clearly increased according to year, especially left side hepatectomy. Rt = right side hepatectomy; Lt = left side hepatectomy.

Fig. 2
(A) CT finding of a large hemangioma occupying central and left liver. The red line indicates transection plane of left trisegmentectomy. (B) CT finding of a large hepatocellular carcinoma occupying right posterior segment. The red line indicates transection plane of right posterior segmentectomy with middle hepatic vein. (C) CT finding of a large hepatocellular carcinoma occupying right liver. The red line indicates transection plane of right trisegmentectomy. (D) CT finding of a large hepatocellular carcinoma occupying left liver. The red bidirectional arrow indicates transection plane of left lobectomy+caudate lobe with Middle hepatic vein. The black unidirectional arrow indicates transaction plane of left loectomy with middle hepatic vein.
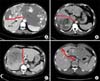
Fig. 3
Various direction of hanging tape during various hepatectomy. (A) The 'a' tape was used during right lobectomy or left lobectomy+caudate lobe with middle hepatic vein. The 'b' tape was used during right posterior segmentectomy with middle hepatic vein or left trisegmentectomy. The 'c' tape was used during right trisegmentectomy. (B) Direction of hanging tape during left lobectomy with middle hepatic vein or right hepatectomy with caudate lobe.



References
1. Yamamoto M, Takasaki K, Ohtsubo T, Katsuragawa H, Fukuda C, Katagiri S. Effectiveness of systematized hepatectomy with Glisson's pedicle transection at the hepatic hilus for small nodular hepatocellular carcinoma: retrospective analysis. Surgery. 2001. 130:443–448.
2. Torzilli G, Leoni P, Gendarini A, Calliada F, Olivari N, Makuuchi M. Ultrasound-guided liver resections for hepatocellular carcinoma. Hepatogastroenterology. 2002. 49:21–27.
3. Takasaki K. Glissonean pedicle transection method for hepatic resection: a new concept of liver segmentation. J Hepatobiliary Pancreat Surg. 1998. 5:286–291.
4. Takasaki K. Hepatic resection using glissonean pedicle transection. Nippon Geka Gakkai Zasshi. 1998. 99:245–250.
5. Lai EC, Fan ST, Lo CM, Chu KM, Liu CL. Anterior approach for difficult major right hepatectomy. World J Surg. 1996. 20:314–318.
6. Liu CL, Fan ST, Cheung ST, Lo CM, Ng IO, Wong J. Anterior approach versus conventional approach right hepatic resection for large hepatocellular carcinoma: a prospective randomized controlled study. Ann Surg. 2006. 244:194–203.
7. Liu CL, Fan ST, Lo CM, Tung-Ping Poon R, Wong J. Anterior approach for major right hepatic resection for large hepatocellular carcinoma. Ann Surg. 2000. 232:25–31.
8. Belghiti J, Guevara OA, Noun R, Saldinger PF, Kianmanesh R. Liver hanging maneuver: a safe approach to right hepatectomy without liver mobilization. J Am Coll Surg. 2001. 193:109–111.
9. Hwang S, Lee SG, Lee YJ, Kim KH, Ahn CS, Kim KW, et al. Modified liver hanging maneuver to facilitate left hepatectomy and caudate lobe resection for hilar bile duct cancer. J Gastrointest Surg. 2008. 12:1288–1292.
10. Kim SH, Park SJ, Lee SA, Lee WJ, Park JW, Kim CM. Isolated caudate lobectomy using the hanging maneuver. Surgery. 2006. 139:847–850.
11. Suh KS, Lee HJ, Kim SH, Kim SB, Lee KU. Hanging maneuver in left hepatectomy. Hepatogastroenterology. 2004. 51:1464–1466.
12. Tanaka S, Taira K, Kudo A, Nakamura N, Ito K, Arii S. Anterior approach for left-sided hepatic resection. Hepatogastroenterology. 2008. 55:1760–1763.
13. Nanashima A, Sumida Y, Abo T, Takeshita H, Hidaka S, Sawai T, et al. Trisectionectomy for large hepatocellular carcinoma using the liver hanging maneuver. Eur J Surg Oncol. 2009. 35:326–330.
14. Hwang S, Lee SG, Ha TY, Ahn CS, Park KM, Kim KH, et al. Simplified standardized technique for living donor liver transplantation using left liver graft plus caudate lobe. Liver Transpl. 2004. 10:1398–1405.
15. Takatsuki M, Kawashita Y, Eguchi S, Tajima Y, Kanematsu T. Tape-guided living donor left hepatectomy. Am J Surg. 2007. 194:107–109.
16. Liddo G, Buc E, Nagarajan G, Hidaka M, Dokmak S, Belghiti J. The liver hanging manoeuvre. HPB (Oxford). 2009. 11:296–305.
17. Nanashima A, Sumida Y, Abo T, Nagayasu T, Sawai T. Usefulness and application of the liver hanging maneuver for anatomical liver resections. World J Surg. 2008. 32:2070–2076.
18. Ogata S, Belghiti J, Varma D, Sommacale D, Maeda A, Dondero F, et al. Two hundred liver hanging maneuvers for major hepatectomy: a single-center experience. Ann Surg. 2007. 245:31–35.
19. Trotovsek B, Belghiti J, Gadzijev EM, Ravnik D, Hribernik M. Anatomical basis of the liver hanging maneuver. Hepatogastroenterology. 2005. 52:728–730.
20. Tsuruta K, Okamoto A, Toi M, Saji H, Takahashi T. Impact of selective Glisson transection on survival of hepatocellular carcinoma. Hepatogastroenterology. 2002. 49:1607–1610.
21. Kim SH, Park SJ, Lee SA, Lee WJ, Park JW, Hong EK, et al. Various liver resections using hanging maneuver by three glisson's pedicles and three hepatic veins. Ann Surg. 2007. 245:201–205.
22. Hashikura Y, Kawasaki S. Living donor liver transplantation: issues regarding left liver grafts. HPB (Oxford). 2004. 6:99–105.
 XML Download
XML Download