

 PDF
PDF ePub
ePub Citation
Citation Print
Print


Abstract
Purpose
Laparoscopy assisted distal gastrectomy (LADG) has been accepted as the best standard operative technique in early gastric cancer. But, no predictive indicators of reconstructive procedure were reported. Analyzing the reconstructive procedure after LADG according to location of the lesion, we, herein, suggest an alternative.
Methods
From May 2008 to May 2009, 55 patients with distal gastric cancer who underwent LADG were examined retrospectively. The group of 55 patients were assigned to two groups according to the reconstructive procedure undertaken: 41, Billroth I (BI); 14, Billroth II (BII). After measuring the distance between esophagogastric junction and tumor (ET) and between pyloric ring and tumor (PT), we found ET/(ET+PT).
Results
The mean±standard error time of ET in BI and BII group was 20.5±7.9 cm (5~38) and 13.9±6.7 cm (6~30). The mean±standard error time of PT in BI and BII group was 15.1±8.2 cm (2~36) and 22.6±9.1 cm (8~40). The mean±standard error time of ET/(ET+PT) in BI and BII group was 57.0±21.1% (16.1~95.0) and 39.1±19.0% (13.0~75.0). ET, PT and ET/(ET+PT) were correlated with reconstructive procedure (P=0.007, 0.006, 0.005). In comparative analysis of correlation between ET and reconstructive procedure, 95% confidence level in BI and BII group is 18.0~22.9 cm and 10.0~17.7 cm; between PT and reconstructive procedure, 12.5~17.7 cm and 17.4~27.8 cm; and between ET/(ET+PT) and reconstructive procedure, 51.1~64.4% and 28.1~50.0%.
Figures and Tables
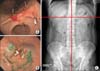 | Fig. 1(A) Endoscopic clipping at proximal and distal margin of the lesion. (B) Endoscopic tattooing on submucosa of the lesion. (C) X-ray finding after endoscopic clipping.
|
 | Fig. 2Relation between distance of the tumor from the esophagogastric junction (ET) and reconstructive procedure.
|

 | Fig. 4Relation between the proportion of distance of the tumor from esophagogastric junction (ET) to total length of the stomach (ET+PT) and reconstructive procedure.
|


References
1. Park CH, Song KY, Kim SN. Treatment results for gastric cancer surgery: 12 years' experience at a single institute in Korea. Eur J Surg Oncol. 2008. 34:36–41.
2. Korea Gastric Cancer Association. Nationwide gastric cancer report in Korea. J Korean Gastric Cancer Assoc. 2002. 2:105–114.
3. The Information Committee of the Korean Gastric Cancer Association. 2004 Nationwide gastric cancer report in Korea. J Korean Gastric Cancer Assoc. 2007. 7:47–54.
4. Sowa M, Kato Y, Nishimura M, Kubo T, Maekawa H, Umeyama K. Surgical approach to early gastric cancer with lymph node metastasis. World J Surg. 1989. 13:630–636.
5. Kim JP, Hur YS, Yang HK. Lymph node metastasis as a significant prognostic factor in early gastric cancer: analysis of 1,136 early gastric cancers. Ann Surg Oncol. 1995. 2:308–313.
6. Hyung WJ, Cheong JH, Kim J, Chen J, Choi SH, Noh SH. Analyses of prognostic factors and gastric cancer specific survival rate in early gastric cancer patients and its clinical implication. J Korean Surg Soc. 2003. 65:309–315.
7. Lim KH, Chung HY, Yu W. Prognosis of early gastric cancer: impact of lymph node metastasis. J Korean Surg Soc. 2003. 65:18–22.
8. Kitano S, Iso Y, Moriyama M, Sugimachi K. Laparoscopy-assisted Billroth I gastrectomy. Surg Laparosc Endosc. 1994. 4:146–148.
9. Japan Society for Endoscopic Surgery. Nationwide survey on endoscopic surgery in Japan. J Jpn Soc Endosc Surg. 2004. 9:475–563.
10. Kim HH, Kim KH, Kim DH, Kim C, Kim BS, Kim YW, et al. Korean Laparoscopic Gastrointestinal Surgery Study Group. Nationwide survey of laparoscopic gastric surgery in Korea, 2004. J Korean Gastric Cancer Assoc. 2005. 5:295–303.
11. Song KY. The current status and future perspectives of laparoscopic surgery for gastric cancer. Korean J Gastroenterol. 2007. 50:233–241.
12. Adachi Y, Shiraishi N, Shiromizu A, Bandoh T, Aramaki M, Kitano S. Laparoscopy-assisted Billroth I gastrectomy compared with conventional open gastrectomy. Arch Surg. 2000. 135:806–810.
13. Song KY, Kim SN, Park CH. Laparoscopy-assisted distal gastrectomy with D2 lymph node dissection for gastric cancer: technical and oncologic aspects. Surg Endosc. 2008. 22:655–659.
14. Ko YJ, Choi SY, Kim CS. A clinical review of laparoscopic surgery in duodenal ulcer. J Korean Surg Soc. 1995. 48:494–501.
15. Kim EK, Lee IK, Kim WW, Chun SW, Kim SN, Song YT. Laparoscopic resection of benign gastric tumor. J Korean Soc Endosc Laparosc Surg. 1998. 1:5–11.
16. Jeong HS, Kim KJ, Cha YJ, Kim SP, Kim GC, Jang JH, et al. Comparison of the early postoperative results after a Billroth I and a Billroth II gastrectomy for gastric cancer. J Korean Gastric Cancer Assoc. 2002. 2:96–100.
17. Kyzer S, Binyamini Y, Melki Y, Ohana G, Koren R, Chaimoff C, et al. Comparative study of the early postoperative course and complications in patients undergoing Billroth I and Billroth II gastrectomy. World J Surg. 1997. 21:763–767.
18. Kojima K, Yamada H, Inokuchi M, Kawano T, Sugihara K. A comparison of Roux-en-Y and Billroth-I reconstruction after laparoscopy-assisted distal gasrectomy. Ann Surg. 2008. 247:962–967.
19. Kim MH, Yoo CH, Sohn CI, Park DI, Jeon WK. Comparative study of duodenogastric reflux according to reconstructive procedure after distal subtotal gastrectomy. J Korean Surg Soc. 2006. 71:256–261.
20. Kim SG, Kim YK, Heo YJ, Song KY, Kim JJ, Jin HM, et al. Comparison of the results in gastric carcinoma patients undergoing Billroth I and Billroth II gastrectomiesy. J Korean Gastric Cancer Assoc. 2007. 7:16–22.
21. Ishikawa M, Kitayama J, Kaizaki S, Nakayama H, Ishigami H, Fujii S, et al. Prospective randomized trial comparing Billroth I and Roux-en-Y procedures after distal gastrectomy for gastric carcinoma. World J Surg. 2005. 29:1415–1421.
22. Fukuhara K, Osugi H, Takada N, Takemura M, Higashino M, Kinoshita H. Reconstructive procedure after distal gastrectomy for gastric cancer that best prevents duodenogastroesophageal reflux. World J Surg. 2002. 26:1452–1457.
23. Csendes A, Burgos AM, Smok G, Burdiles P, Braghetto I, Diaz JC. Latest results (12-21 years) of a prospective randomized study comparing Billroth II and Roux-en-Y anastomosis after a partial gastrectomy plus vagotomy in patients with duodenal ulcers. Ann Surg. 2009. 249:189–194.
 XML Download
XML Download