

 PDF
PDF ePub
ePub Citation
Citation Print
Print


Abstract
Purpose
Conventional total gastrectomy with Roux-en-Y esophagojejunostomy has certain limitations such as insufficient food reservoir and malabsorption of nutrients. Therefore, we performed reconstruction of the jejunal pouch interposition (JPI) after near-total gastrectomy preserving the lower esophageal sphincter (LES). We compared the technical feasibility, safety, and surgical outcome of this operation with conventional total gastrectomy accompanying with Roux-en-Y esophagojejunostomy.
Methods
From April 2003 to October 2005, 15 LES-preserving, near-total gastrectomies with JPI (LES-JPI group) were performed. The clinical features and surgical outcomes were retrospectively compared with 17 cases of conventional R-Y esophagojejunostomy. Statistical analysis was performed using Fisher's exact test for categorical data and an unpaired t-test for continuous data.
Results
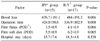
Clinicopathological features of the LES-JPI and R-Y groups did not show differences excepting patient age (50.8±5.8 years vs. 62.8±12.4, respectively; P=0.002) and the depth of tumor invasion (T1-T2; 11~4 vs. 5~12; P=0.032). The operative outcomes for the two groups significantly differed in terms of operation time (676 vs. 484 min; P=0.008) and blood loss (424 vs. 336 ml; P=0.006). Postoperative gastrofiberscopic examination of all LES-JPI patients showed no esophageal reflux or strictures and intact LES. In addition, the LES-JPI group did not experience swallowing difficulty or stricture.
Figures and Tables
Fig. 1
Proximal resection. Auto-purse string device is applied for proximal resection at a distance of 1.5 to 2.5 cm from the lower esophageal sphincter.

Fig. 2
Jejunal pouch reconstruction. Jejunal pouch is reconstructed in a side-to-side manner, using a 100-mm GIA stapler. (A) Application of a GIA device. (B) Completion of a jejunal pouch.

Fig. 3
Anastomosis. Jejunal pouch is anastomosed between proximal cardia and duodeneum. (A) An illustration. (B) An upper gastrointestinal contrast test.
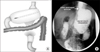
Fig. 4
Comparision of perioperative changes in nutritional markers. The groups showed no statistically significant differences in terms of (A) total protein, albumin, or (B) prognostic nutritional index. P-values refer to the differences in the change of the nutritional markers from their preoperative level between the two groups.

Fig. 5
A comparison of the proportion of body weight loss relative to preoperative body weight. Postoperative weight loss in the LES-JPI group (8.70~9.12%) was lower than that in the R-Y group (10.57~14.13%), the difference was not statistically significant. P-values refer to the differences in the change of the weight from their preoperative level between the two groups.



References
1. Bradley EL 3rd, Isaacs J, Hersh T, Davidson ED, Millikan W. Nutritional consequences of total gastrectomy. Ann Surg. 1975. 182:415–429.
2. Hunt CJ. Construction of food pouch from segment of jejunum as substitute for stomach in total gastrectomy. AMA Arch Surg. 1952. 64:601–608.
3. Lawrence W Jr. Reservoir construction after total gastrectomy: an instructive case. Ann Surg. 1962. 155:191–198.
4. Scott HW Jr, Law DH 4th, Gobbel WG Jr, Sawyers JL. Clincal and metabolic studies after total gastrectomy with a Hunt-Lawrence jejunal food pouch. Am J Surg. 1968. 115:148–156.
5. Takeshita K, Sekita Y, Tani M. Medium- and long-term results of jejunal pouch reconstruction after a total and proximal gastrectomy. Surg Today. 2007. 37:754–761.
6. Nozoe T, Anai H, Sugimachi K. Usefulness of reconstruction with jejunal pouch in total gastrectomy for gastric cancer in early improvement of nutritional condition. Am J Surg. 2001. 181:274–278.
7. Stael von Holstein C, Ibrahimbegovic E, Walther B, Akesson B. Nutrient intake and biochemical markers of nutritional status during long-term follow-up after total and partial gastrectomy. Eur J Clin Nutr. 1992. 46:265–272.
8. Kim W, Jeon HM, Hur H, Lee JH, Won JM. Jejunal pouch interposition after distal gastrectomy in patients with gastric cancer. J Korean Gastric Cancer Assoc. 2004. 4:242–251.
9. Takeyoshi I, Ohwada S, Ogawa T, Kawashima Y, Ohya T, Kawate S, et al. Esophageal anastomosis following gastrectomy for gastric cancer: comparison of hand-sewn and stapling technique. Hepatogastroenterology. 2000. 47:1026–1029.
10. Besson A. The Roux-Y loop in modern digestive tract surgery. Am J Surg. 1985. 149:656–664.
11. Collard JM, Romagnoli R. Roux-en-Y jejunal loop and bile reflux. Am J Surg. 2000. 179:298–303.
12. Herfarth C, Stern J, Buhl K. Small intestine pouches as a therapeutic principle in stomach and large intestine replacement. Z Gastroenterol. 1988. 26:397–403.
13. Miyoshi K, Fuchimoto S, Ohsaki T, Sakata T, Ohtsuka S, Takakura N. Long-term effects of jejunal pouch added to Roux-en-Y reconstruction after total gastrectomy. Gastric Cancer. 2001. 4:156–161.
14. Woodward A, Sillin LF, Bortoff A. Migrating myoelectric complex and jejunal slow-wave propagation after Roux gastrectomy in dogs. Dig Dis Sci. 1993. 38:1073–1078.
15. Karlstrom LH, Soper NJ, Kelly KA, Phillips SF. Ectopic jejunal pacemakers and enterogastric reflux after Roux gastrectomy: effect of intestinal pacing. Surgery. 1989. 106:486–495.
16. Zherlov G, Koshel A, Orlova Y, Zykov D, Sokolov S, Rudaya N, et al. New type of jejunal interposition method after gastrectomy. World J Surg. 2006. 30:1475–1480.
17. Miholic J, Meyer HJ, Muller MJ, Weimann A, Pichlmayr R. Nutritional consequences of total gastrectomy: the relationship between mode of reconstruction, postprandial symptoms, and body composition. Surgery. 1990. 108:488–494.
18. Del Gaudio A, Marzo C. Interposition of the first jejunal loop for reconstruction after total gastrectomy. Int Surg. 1991. 76:91–97.
19. Schwarz A, Buchler M, Usinger K, Rieger H, Glasbrenner B, Friess H, et al. Importance of the duodenal passage and pouch volume after total gastrectomy and reconstruction with the Ulm pouch: prospective randomized clinical study. World J Surg. 1996. 20:60–66.
20. Yasoshima T, Denno R, Ura H, Mukaiya M, Yamaguchi K, Hirata K. Development of an ulcer in the side-to-side anastomosis of a jejunal pouch after proximal gastrectomy reconstructed by jejunal interposition: report of a case. Surg Today. 1998. 28:1270–1273.
21. Iivonen MK, Ahola TO, Matikainen MJ. Bacterial overgrowth, intestinal transit, and nutrition after total gastrectomy. Comparison of a jejunal pouch with Roux-en-Y reconstruction in a prospective random study. Scand J Gastroenterol. 1998. 33:63–70.
 XML Download
XML Download