

 PDF
PDF ePub
ePub Citation
Citation Print
Print


INTRODUCTION
The urachus is a remnant of the primitive bladder and is a homologue of median umbilical ligament in adults.(1) It would be presented as a patent urachus, a urachal cyst, a vesicourachal diverticulum, or a urachal sinus. The urachal cyst is the most common type with an incidence of 1 in 5,000.(2) It can be found incidentally without any symptoms, but infection or discharge can be encountered with it. The treatment is complete surgical excision of it for preventing infectious complications and infrequent occurrence of malignancy.(3) Since it is located beneath the posterior rectus muscular sheath, a lower midline abdominal incision is required for the resection during the conventional open surgery. Laparoscopic approach to the resection has been performed since the early 1990s,(4,5) and the wound-related complications, postoperative pain and a long linear scar on abdominal wall have been minimized by the laparoscopic surgery. According to the previous reports, most of the laparoscopic surgeries were performed by a transabdominal approach, and therefore, intestinal adhesion to the opened parietal peritoneum and multiple upper abdominal scars for trocars could be ineludible, as was found in the transabdominal laparoscopic herniorrhaphy.(6-8) With this condition, a totally extraperitoneal approach would be beneficial, and we are to describe a successful case of laparoscopic excision of urachal cyst by a total extraperitoneal approach.
CASE REPORT
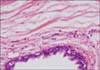
A 39-year-old male patient was referred for a mild abdominal pain without fever for a few days. There was no palpable mass on the physical examination, but the ultrasonography and computerized tomogram revealed a 4.2 cm-sized tubular structure between the bladder and the umbilicus. Laparoscopic preperitoneal approach was planned and the patient was placed in the supine position under general anesthesia. First, a transverse incision was made below the umbilicus, which was deepened to the anterior and the posterior sheath of rectus muscle on the left side of the linea alba to meet the lateral side of the urachal cyst. The opening was widened using the long Kelly clamps, and when the attachment of the urachal cyst was palpated by finger, the 12 mm trocar for a 30-degree laparoscope was inserted. The preperitoneal space was created by the direct telescopic dissection method as was used in totally extraperitoneal herniorrhaphy (TEP).(7) When the bladder and its attached part to the urachal cyst was reached, an additional 12 mm trocar was inserted in the suprapubic area and further dissection was performed around the bladder wall (Fig. 1). A Hem-o-Lok® (Weck Closure Systems, Durham, NC, USA) clip was applied between the cyst and the bladder, and the cyst was divided. The urachal cyst was pulled out through the infraumbilical incision and divided from its umbilical attachment (Fig. 2). The fascias of rectus muscle in port sites were repaired using absorbable suture, and the skin incision was closed. The patient was discharged on the first postoperative day and the pathologic examination revealed urachal cyst without malignancy (Fig. 3).
DISCUSSION
The urachus, an embryonic remnant structure, is located beneath the transversalis fascia and is bordered by the obliterated umbilical arteries on both sides. The conventional open surgery on it accompanies the division of linea alba in the lower abdominal wall with or without peritoneal injury. Although laparoscopic approach shown in the previous studies made it possible to minimize a long vertical incisional scar and the related complications, the procedure was difficult and additional complications could still exist. During the transabdominal laparoscopic approach, three or more trocars were required and at least two of those were located in the upper abdomen. The videoscopic camera could not be located in the umbilical area as is in other laparoscopic surgeries, and the trocars for operator were located on the lateral abdominal wall. During the operation, the dissection would be performed on the anterior abdominal wall (or the ceiling of the abdominal cavity) with laterally approaching instruments, which is the reverse direction of usual laparoscopic surgery performed on colon or other abdominal organs. The hospital stay of the patients treated with transabdominal laparoscopic approach was three to five days.(4,5,9)
On the other hand, for the extraperitoneal laparoscopic approach in our case, there requires only two trocars on the lower abdomen (the one in the infraumbilical area, and the other in the suprapubic area). Moreover, peritoneum was preserved during the operation and the possibility of intraabdominal organ injury and intestinal adhesion after operation was decreased. The hospital stay was only one day after the operation in this report, which is as similar as that of TEP.(10)
There are certain differences between TEP and extraperitoneal urachal cyst resection. Extraperitoneal dissection was started beneath the transversalis fascia in urachal cyst rather than above the posterior rectus muscular sheath in TEP. It results that the peritoneum between umbilicus and the semilular line of posterior rectus muscular sheath is more vulnerable to injury. On the other hand, the operative visual field in this case is better than that in TEP.
To date, the laparoscopic surgery for urachal anomalies was reported in a limited number of cases and it is difficult to evaluate the efficacy and safety based on controlled studies. However, with minimal injury on normal tissue and early recovery after operation, the extraperitoneal approach would be a good surgical option for the treatment of urachal cyst.


 XML Download
XML Download