

 PDF
PDF ePub
ePub Citation
Citation Print
Print


INTRODUCTION
The use of endovascular aortic aneurysm repair (EVAR) has expanded ever since the first EVAR was introduced in 1991. The mortality rate of abdominal aortic aneurysm (AAA) repair has recently improved in proportion to increased use of EVAR.(1) However, the rate of secondary interventions due to endograft failure such as endoleaks, migration or graft occlusion was reported to be 16.2% on a previous meta-analysis.(2) The delayed open conversion rate after EVAR ranges from 0.6% to 4.5%.(3,4) Even though the open conversion rate is decreasing with advancement of endovascular technique and development of a new generation of stent grafts, open conversion is still required, occasionally. Open conversion is somewhat different from primary open repair and it is technically challenging. We report here on our experience with two cases of delayed open conversion that were due to type III endoleak.
CASE REPORT
1) Case 1
A 70-year-old man presented with an asymptomatic abdominal pulsating mass. Computed tomography (CT) showed 6.0 cm AAA with bilateral common iliac artery (CIA) aneurysms. He had a history of extensive bilateral pulmonary emphysema and coronary artery disease. He underwent staged bilateral hypogastric artery embolizations, and then had a Vanguard endovascular stent graft (Boston Scientific, Natick, MA, USA) placed. At 45 months after EVAR, follow-up CT revealed that the left limb was separated from the main body (type III endoleak, Fig. 1). Elective open conversion was planned. Through transperitoneal approach, infrarenal aortic cross clamping was applied and aneurysm sac was opened. The left limb was disconnected from main body. The stent graft was easily removed because there was no firm adherence of the stent graft to the aorta and the iliac arteries. In situ aortic reconstruction using a bifurcated PTFE graft was performed. Aortic clamping time was 90 minutes and estimated blood loss was 4,000 ml. He received ventilator therapy for 5 days postoperatively and then he was discharged on postoperative day 17.
2) Case 2
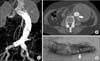
A 78-year-old woman presented with an abdominal pulsating mass. Eight years earlier, she had stent graft placed for 6-cm AAA at another hospital and an additional bare stent was placed on the proximal aneurysmal neck to seal a type I endoleak. Six years ago, CT showed the presence of a type III endoleak on the posterior aspect of the distal main body and the diameter of AAA was 6.6 cm. We recommended secondary open repair, but she declined and was lost to follow-up. She revisited our hospital 6 years later complaining of an abdominal mass that was increasing in size on her left flank. She denied any abdominal or back pain. CT revealed a 9.9 cm sized AAA with a persistent type III endoleak and she underwent elective open conversion (Fig. 2). Through transperitoneal approach, aneurysm was exposed. The proximal stent tip was palpated 1 cm inferior to the renal artery. After left renal vein division, infrarenal aortic cross clamping was done just below the level of the renal arteries and the aneurysm sac was opened. The aortic wall interfacing with the stent graft was thin and there was dense adhesion between the stent graft and the aorta. It was very hard to detach the stent graft from the aortic wall and the iliac wall. We transected the aorta at the level of the bare stent and cut the stent with wire cutter. Both iliac limbs were also transected at the proximal CIA level and both CIAs were oversewn. We left the proximal bare stent and both distal iliac limbs in place. The stent graft was home-made and showed a large defect on the suture line between the main body and the left distal limb. A bifurcated PTFE graft was used for aortic reconstruction. Proximal anastomosis was made on the infrarenal aorta and distal anastomoses were performed on the bilateral external iliac arteries (EIAs) in an end-to-side fashion. Aortic clamping time was 130 minutes and estimated blood loss was 11,000 ml. She was discharged without any complication on postoperative day 10.
DISCUSSION
Type III endoleak is defined by the persistence of blood flow outside the lumen of endograft from module disconnection or fabric disruption and its incidence was reported as 4.2%.(2) For the treatment of a late type III endoleak, endovascular or hybrid treatment such as deployment of another endograft,(5) placement of an aortomonoiliac device and a contralateral iliac plug followed by a femoro-to-femoral bypass,(6) can be considered. However, an aorto-monoiliac graft is currently not available in Korea.
The first issue in delayed open conversion is aortic control. Fortunately, infrarenal aortic clamping was possible in our cases because both endografts were not suprarenal fixating type and there was infrarenal uncovered native proximal aortic neck. Suprarenal or supraceliac aortic control is needed in some cases, and especially when using a suprarenal fixating devices. It is well known that prolonged suprarenal aortic control increases the perioperative mortality.(7) To improve the outcome, some authors have used suprarenal aortic ballooning instead of suprarenal aortic cross clamping.(8) Suprarenal balloon inflation was applied for vascular control and then infrarenal aortic cross clamping was followed after removing the stent's metal barbs or hooks. To remove suprarenal fixating stent graft, it is needed to cut suprarenal fixating bare stent. However, it is not necessary to remove a bare stent portion. It can be left in place to reduce suprarenal aortic clamping time.
The second issue is the selection of the anastomotic site. The arterial wall that had contacted with the stent graft, such as the proximal neck or the common iliac artery, is usually thin and the stent is firmly adherent to the arterial wall. McArthur et al.(9) reported 11 cases of histopathologic analysis of endograft. Of the eleven endografts, only 3 were easily removed. Eight were densely adhered to the aortic wall, although they failed to demonstrate evidence of significant stent graft incorporation at anastomotic site on microscopic examination. In our second case, the removal of the endograft was extremely difficult, while the endograft was removed easily in case 1. It was explained by foreign body reaction or an inflammatory response to metal penetration of the arterial wall by hooks.(10) We assumed that oversizing of the stent graft to prevent endoleak was one of the causes. This thinned and inflammatory aortic wall is not appropriate for anastomosis due to risk of anatomotic bleeding. Therefore, it is important to avoid this segment as an anastomotic site. Complete removal of an endograft is not always necessary as long as it is well-incorporated and not infected. It would make an operation complicated and prolong the operation time. Partial removal of an endograft is an alternative. Some authors prefer partial endograft removal in order to allowing a graft-to-graft anastomosis.(8) In the second case, we kept the distal limb in CIA and ligated the CIA stump and made distal anastomoses on the bilateral EIAs that were free from stent grafts instead of graft-to-graft anastomosis. Several modes of anastomosis are illustrated in Fig. 3.
Tips for delayed open conversion are summarized as following:
Do not try to completely remove the bare stent portion or stent graft under the suprarenal aortic clamping.
Avoid anastomosis with a thinned arterial wall that has interfaced with an endograft.
Unless an endograft is easily removed, consider graft-to-graft anastomosis with partial endograft removal.
In conclusion, making a plan for delayed open convertsion should be individualized according to the type and status of the endograft and the vascular anatomy. Whether to perform infrarenal aortic control or suprarenal aortic control, how to control the proximal aorta (e.g. aortic cross clamping or balloon inflation), and whether to completely or partially remove the graft should be considered.


 XML Download
XML Download